
|
|
Graves' disease - Case 19.
|
|

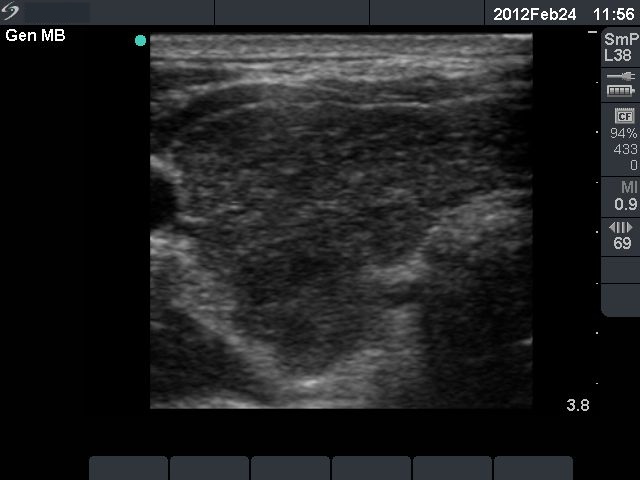

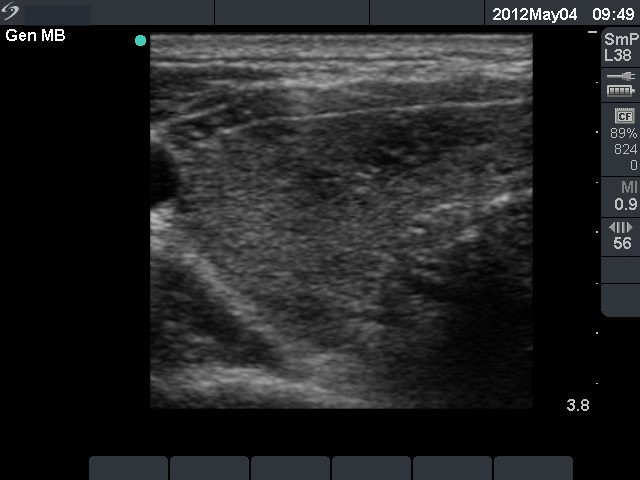



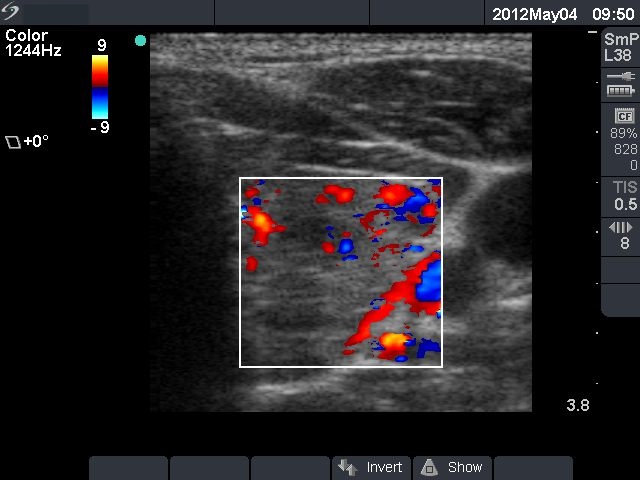


First examination (first row):
Clinical presentation: a 24-year-old man was referred for an evaluation of typical complaints suggesting hyperthyroidism.
Palpation: enlarged thyroid without any nodule.
Functional state: hyperthyroidism with TSH 0.001 mIU/L, FT4 51.2 pM/L.
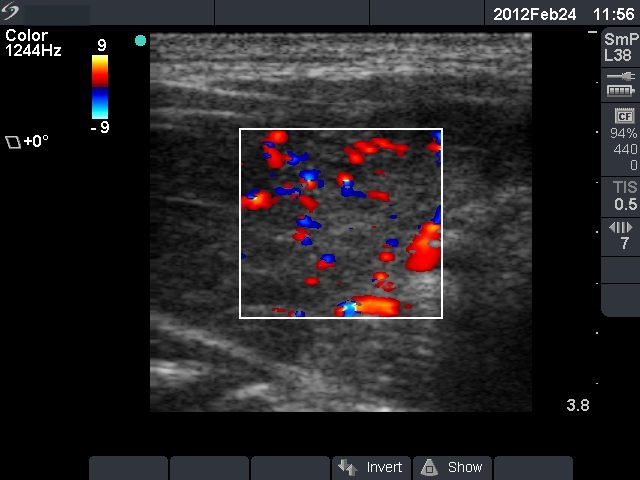
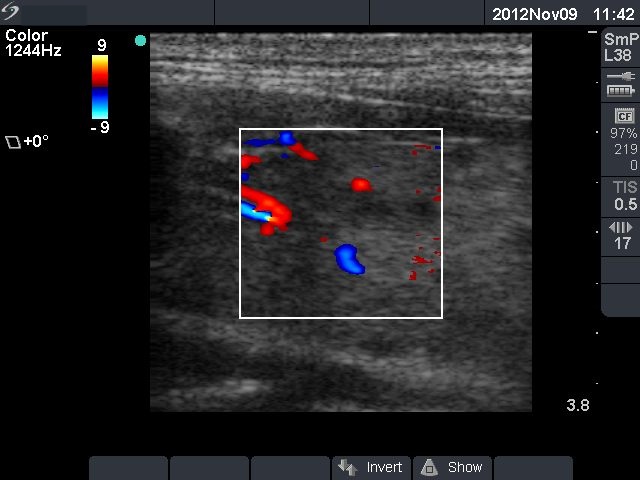
Ultrasonography: the thyroid was hypoechogenic without any nodule. The vascularization was increased.Clinical diagnosis: hyperthyroidism caused by Graves-Basedow's disease.
We administered daily 20 mg methimazole to the patient.
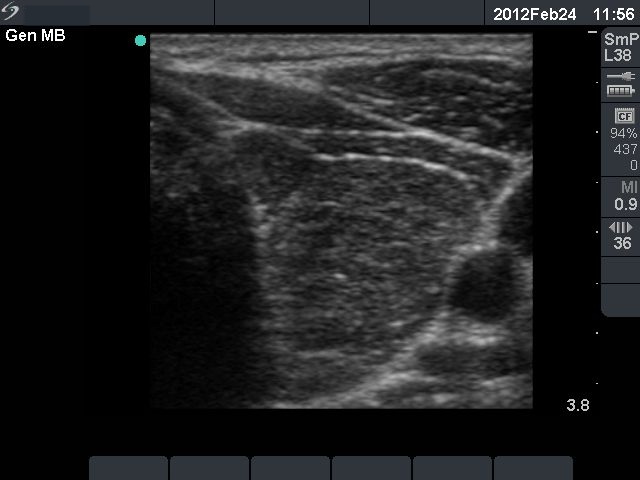
10 weeks after initial investigation (second row):
Clinical presentation: the complaints of the patients have resolved.
Palpation: unchanged.
Functional state: subclinical hyperthyroidism on daily 20 mg methimazole with TSH-level 0.02 mIU/L, FT4 17.5 pM/L.
Ultrasonography: the thyroid was minimally-moderately hypoechogenic. The vascularization was increased.
The dose of the methimazole was decreased to daily 10 mg. The patient was evaluated every 3 months.
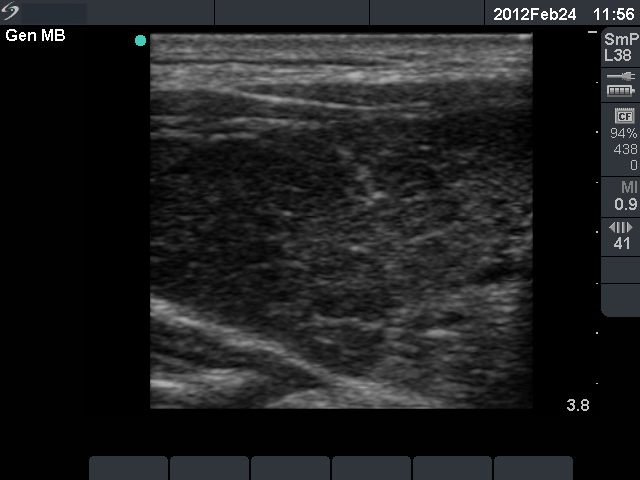
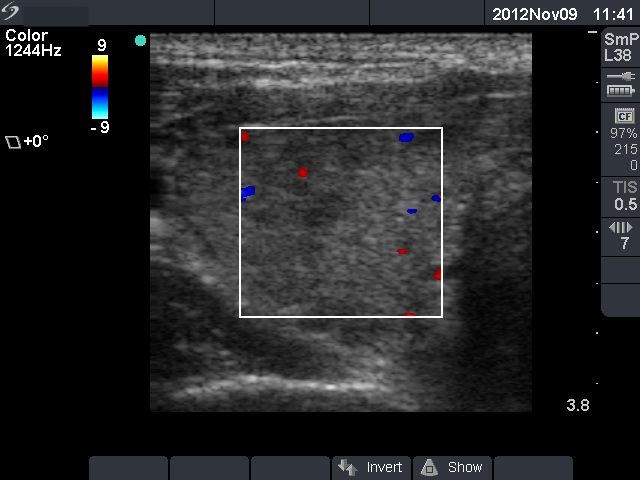
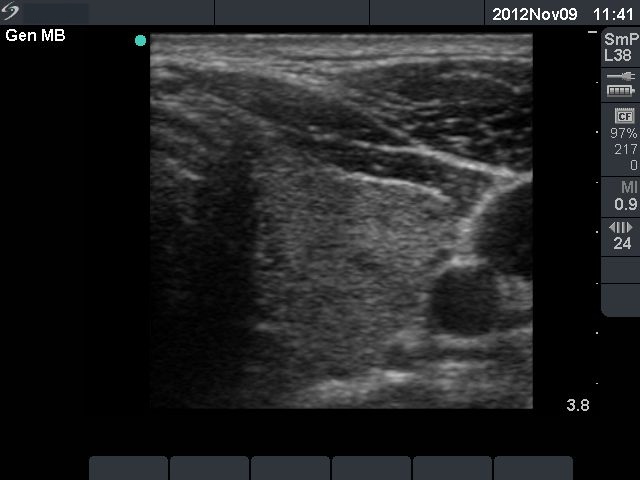
9 months after initial investigation (third row):
Clinical presentation: the patient was well.
Palpation: no abnormality.
Functional state: euthyroidism on daily 5 mg methimazole with TSH-level 0.38 mIU/L, FT4 13.5 pM/L, TSH-receptor antibody test positive.
Ultrasonography: the echo structure and the vascularization of the thyroid became echonormal.
3 months later the methimazole therapy was discontinued.
13 month after discontinuation of methimazole the patient remained euthyroid.