
|
|
Subacute granulomatous de Quervain's thyroiditis - Case 20. |
|






Clinical data: a 43-year-old woman with a multinodular goiter was referred for an evaluation.
Palpation: the right thyroid was enlarged and two nodules were palpable. The left thyroid was tender on palpation.
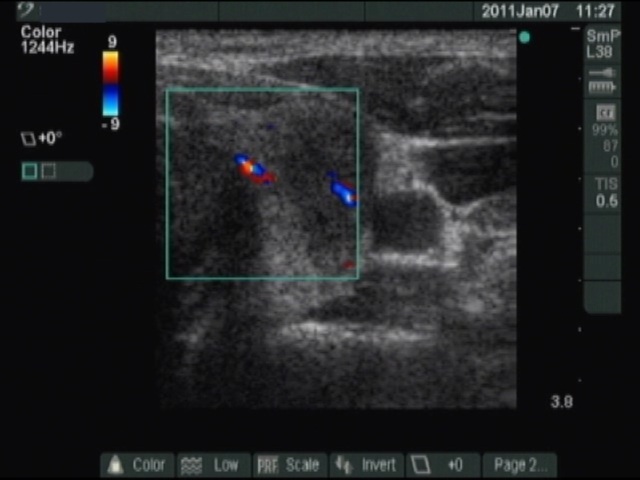
Ultrasonography: there were a hyperechogenic and a moderately hypoechogenic nodule in the enlarged right thyroid, while a hypoechogenic lesion with blurred borders in the left lobe. The vascularization was not specific. (The picture demonstrate the left thyroid.)
After ultrasonography: I asked the patient about neck complaints. She told me that she suffered from upper airways infection 4 weeks earlier and the left side of the neck is tender for a few days. She did not experience subfebrility or fever.
Results of blood test: euthyroidism with subnormal TSH level: TSH 0.11 mIU/L, FT4 14.8 pM/L, FT3 4.55 pM/L.
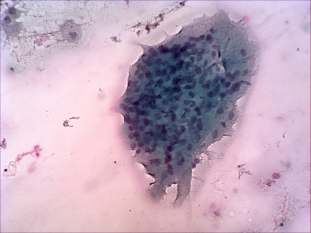
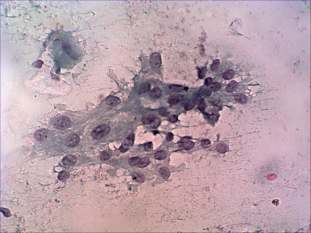
Cytological picture: no colloid in the background. Inflammatory cells mixed with typical and degenerated thyrocytes. Numerous multinucleated giant cells, some of them composed of elongated epitheloid cells.
Cytological diagnosis: benign subacute, granulomatous, de Quervain's thyroiditis.
Accessory blood test: CRP 21.6 mg/L.
Suggestion: we did not prescribe any medical therapy. 6 weeks later the patient had no complaints and the CRP became normal.
Comment: the routine use of ultrasonography altered the diagnostics of de Quervain's thyroiditis. In around 10% of our cases, we diagnose this disease in patients without typical complaints. Therefore, we must be aware of the similarity of the ultrasonographic pattern of de Quervain's thyroiditis and papillary cancer.