
|
|
The role of complex diagnosis - follicular proliferation - Case 1.
|
|









Clinical data: a 40-year-old man visited us. Her wife watched a soap opera on TV, where a man was operated for thyroid cancer. It caused great anxiety because she was known having a thyroid nodule for years. She indicated an examination by herself and her husband. The man had no complaints.
Palpation: a nodule in the right lobe.
Functional state: euthyroidism with TSH-level 1.28 mIU/L.
Ultrasonography: there was an echonormal nodule presenting a halo sign and perinodular blood flow in the right lobe.
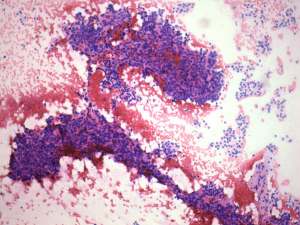
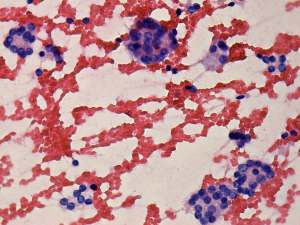
Cytological picture: follicular tumor.
We suggested follow-up examinations instead of surgery because taking the sonographic and the cytological picture into account, the risk of a follicular carcinoma was estimated less than 2%. The wife decided that her husband undergoes an operation.
Histopathology: revealed normofollicular adenoma.
This case is enlisted among Follicular adenomas - case 7, too.