
|
|
Chronic lymphocytic thyroiditis - Case 1.
|
|




Clinical data: a 36-year-old woman was referred for an evaluation of a toxic multinodular goiter. She had palpitation and 5 kg shrinkage.
Palpation: both thyroids were firm. There was a nodule palpable in the isthmus.
Hormonal examination indicated hyperthyroidism with TSH-level 0.001 mIU/L, and FT4 38.9 pM/L.
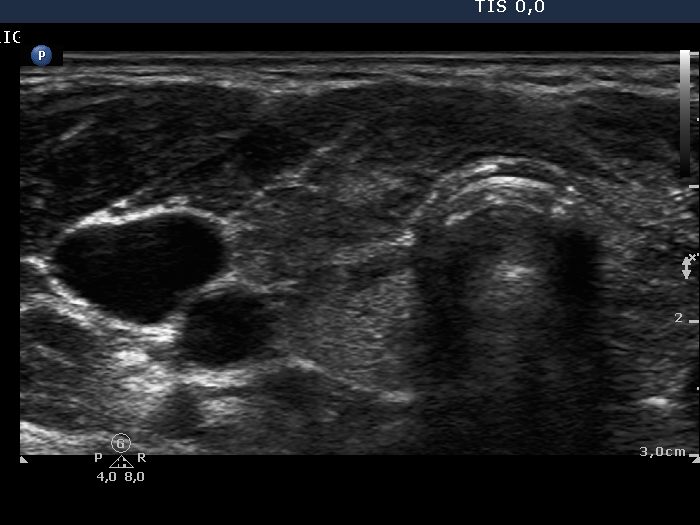
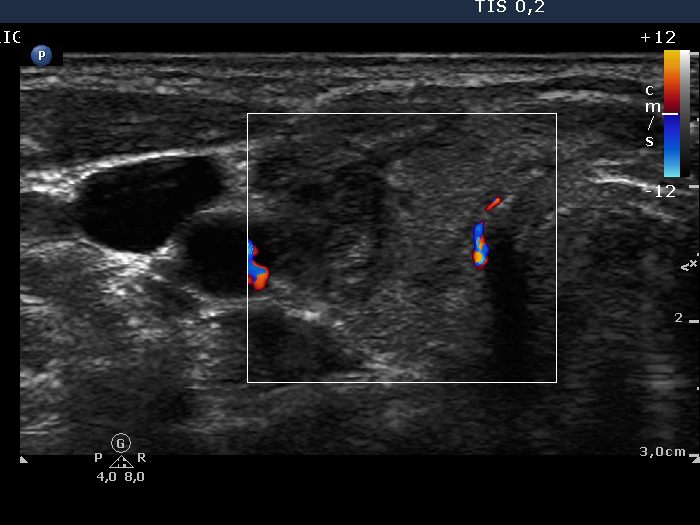
Ultrasonography: the thyroid contained around 40% hypoechogenic discrete lesions. The irregular shape of the lesions and the lack of thyroid enlargement stood for autoimmune thyroid disease, and for Hashimoto's thyroiditis. The presence of nodules in pathological sense was unlikely, but we could not exclude this possibility. The vascularization of the thyroid was decreased. The circumscribed lesion in the right side of the isthmus was aspirated.
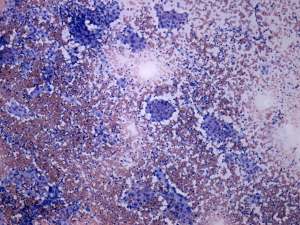
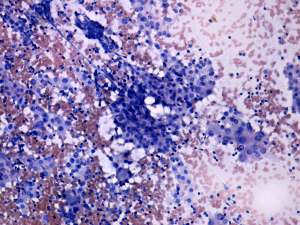
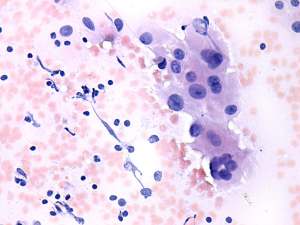
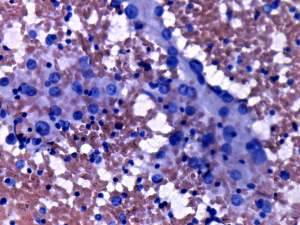
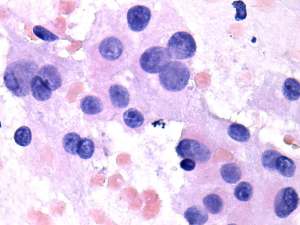
Cytological diagnosis: benign Hashimoto thyroiditis.
Both TsAb and aTPO were in the normal range, the latter resulted in 8 U/mL.
Clinical diagnosis : Hashimoto thyroiditis. Hyperthyroidism caused by hashitoxicosis.
We did not administer thyrostatic drug. 4 weeks later the FT4-level rose to 42.1 pM/L. Thereafter 10 mg methimazole therapy was started. Two weeks later fever developed. Blood test resulted in agranulocytosis with a neutrophil-count below 0.1 G/L (normal value 2-8)) and hypothyroidism (TSH 1.54 mIU/L, FT4 6.09 pM/L).
Antibiotics was started and the methimazole therapy was discontinued. 3 days later the neutrophil count normalized. We suggested radio-iodine therapy, but the iodine-intake was low. The patient was operated.
Histopathology: Hashimoto's thyroiditis without any nodule.
Comments:
-
Even in typical cases of Hashimoto's thyroiditis, the aTPO sensitivity is not greater than 90-95%.
-
In around 1/4 of our patients with hashitoxicosis, the elevated FT4-level did not normalize within a month.
-
Considering the course of the disease, the patient had a great chance avoiding relapse of hyperthyroidism. However, in the case of an agranulocytosis a definitive therapy is mandatory.
-
The ultrasound pattern (the gray scale mode) disclosed autoimmune thyroid disease with great probability. The decreased vascularization in non-nodular form of hyperthyroidism stands against active hormone-producing disease, but argues for hashitoxicosis with great probability.