
|
|
Benign nodular hyperplasia - Case 51.
|
|







Clinical presentation: a 47-year-old woman was referred for evaluation of a multinodular goiter known for 6 years.
Palpation: multiple nodules were palpated. There was a large, firm nodule in the left lobe.
Functional state: euthyroidism (TSH 1.67 mIU/L).
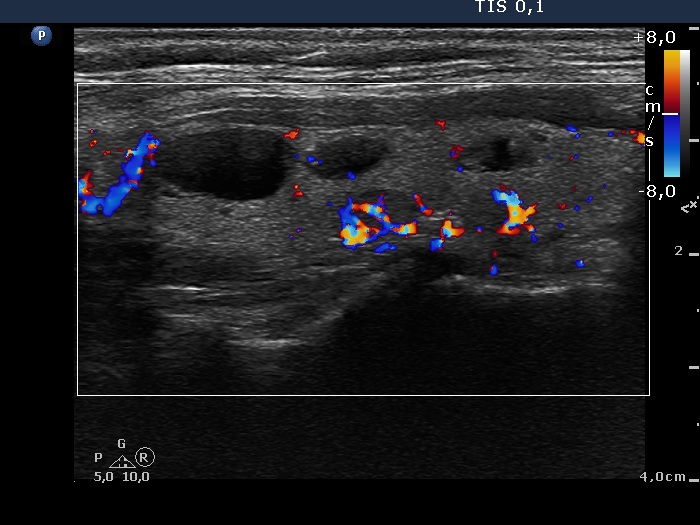
Ultrasonography: The thyroid was echonormal and contained several nodules with different echogenicities including a hypoechogenic one in the ventromedial part of the left lobe. This lesion presented a lobulated margin and a type 1 vascular pattern.
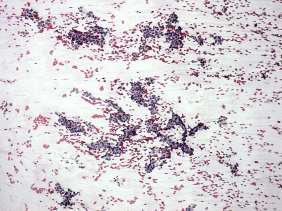
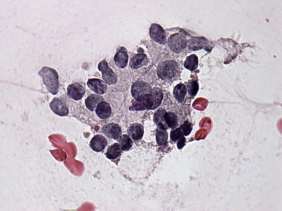
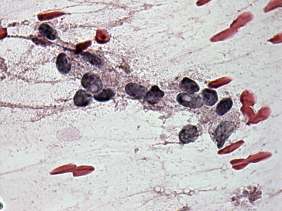
Cytology was performed form the nodule described above. A dominantly microfollicular proliferation was found. A few nuclei presented intranuclear holes and groove-like figures. There were some irregular microfollicles presenting nuclear crowding and loss of polarity of cells.
Considering the lobulated margin of the lesion and the cytological findings, we gave a common ultrasound-cytological diagnosis of suspicion of papillary carcinoma.
The patient underwent left lobectomy. Intraoperative frozen section indicated a benign lesion. Final histopathological result was benign hyperplastic nodules included the suspicious lesion while the larger nodule proved to be a follicular adenoma.
Comment. Although there were cytological signs which were not fully reassuring, the cytological pattern itself is not enough to raise the possibility of a papillary carcinoma. While the cytology might correspond to a follicular tumor, the ultrasound presentation practically excluded the possibility of a follicular carcinoma. The lobulated margin of the lesion was worthy of note. Taking all these into account, we raised the possibility of papillary carcinoma.
By reviewing the ultrasound and cytology, I think that the correct diagnosis would be benign follicular proliferation with not greater than 1% risk of malignancy. The lack of significantly enlarged nuclei is a strong argument against a papillary carcinoma.