
|
|
Graves' disease - Case 27.
|
|







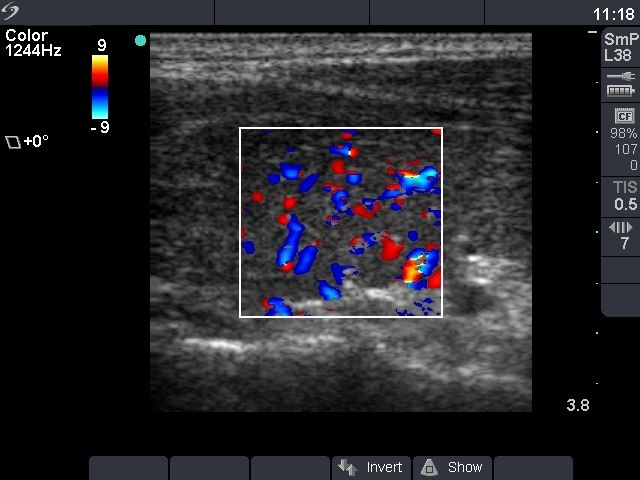

First examination (first row):
Clinical presentation: a 24-year-old man was referred for an evaluation of hyperthyroidism.
Palpation: no abnormality.
Functional state: hyperthyroidism with TSH 0.001 mIU/L, FT4 57.1 pM/L.
Ultrasonography: the thyroid was moderately hypoechogenic without any nodule. The vascularization was increased.Clinical diagnosis: hyperthyroidism caused by Graves-Basedow's disease.
The patient was treated with methimazole for 15 months. Thereafter he had no complaints.
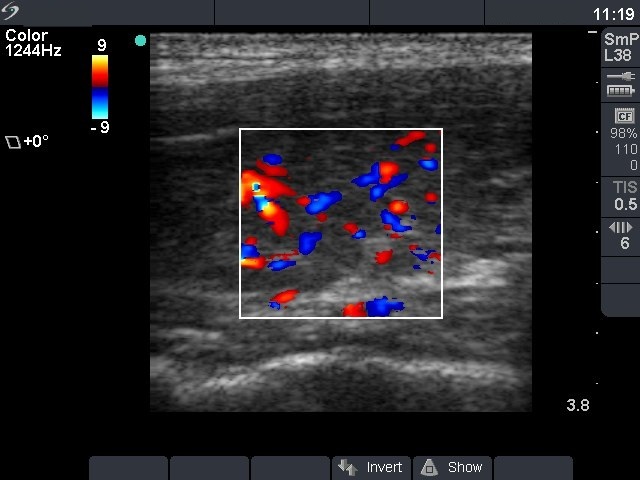
Second examination 4 months later (2nd row):
Clinical presentation: three months after discontinuation of methimazole therapy the patient had complaints suggesting recurrence of the hyperthyroidism.
Palpation: no abnormality.
Functional state: hyperthyroidism with TSH-level 0.02 mIU/L, FT4 33.1 pM/L.
Ultrasonography: the thyroids were hypoechogenic, and the vascularization was increased but not such an extent as observed at the first examination.
Clinical diagnosis: recurrent hyperthyroidism caused by Graves-Basedow's disease.
The patient was treated again with methimazole. 6 weeks later when FT4 level has normalized, the patient underwent radioiodine therapy.