
|
|
Subacute granulomatous de Quervain's thyroiditis - Case 24.
|
|










First examination (1st and 2nd rows of images):
Clinical presentation: a 36-year-old woman was referred for the evaluation of a painful thyroid. She had subfebrility. Her complaints began 2 weeks before the examination. 5 years earlier she has been treated for subacute thyroiditis with steroid therapy.
Palpation: both thyroids were painful.
Functional state: subclinical hyperthyroidism (TSH-level undetectable, FT4 18.7 pM/L, FT3 6.96 pM/L, sedimentation rate 33 mm/H, CRP 9.4 mg/L).
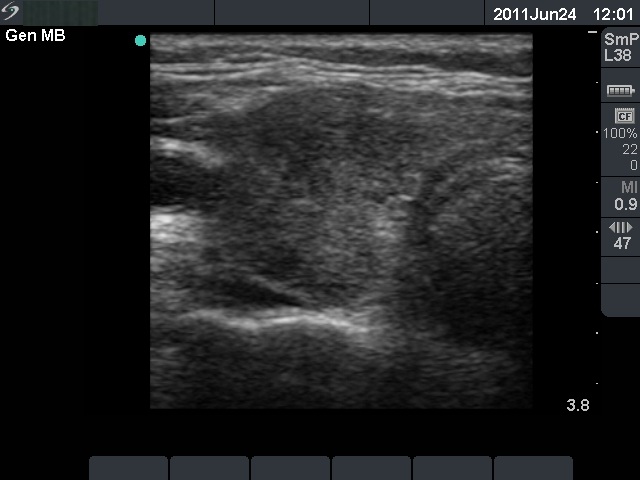
Ultrasonography: the basic echo structure of the thyroid was normal with multiple hypoechogenic lesion with ill-defined borders. The vascularization was decreased.
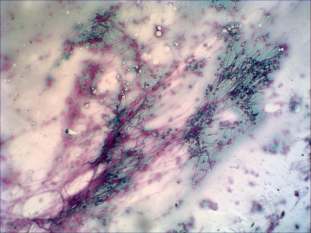
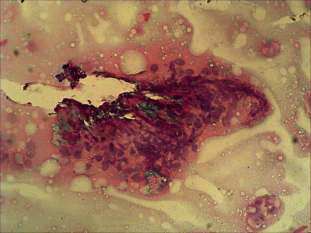
Cytological picture: there was diffuse colloid precipitate in the background. Several multinucleated giant cells, inflammatory cells mixed nuclear debris and clusters of thyrocytes are present on the smear.Cytological diagnosis: subacute, granulomatous de Quervain's thyroiditis.
We performed anti-TPO determination which resulted in normal value, i.e. below 10 IU/mL.
The signs and complaints of the patient suddenly stopped on the day of steroid administration. Both hormonal levels and the ultrasonographic pattern normalized in the follow-up examination.
Follow-up examination 19 months later (3rd row of images):
Clinical presentation: the patient had no complaints.
Palpation: no abnormality.
Functional state: subclinical hyperthyroidism (TSH 1.96 mIU/L, FT4 13.6 pM/L, sedimentation rate 2 mm/H, CRP 1.38 mg/L).
Ultrasonography: the thyroid became echonormal.
Comment: there were two very unusual circumstances in this case. Firstly, de Quervain's thyroiditis is a self-limiting disorder, which extremely rarely appears again after the onset. We found this happening in only two of the first 500 patients with this disease. Secondly, the clinical picture imitated post partum lymphocytic thyroiditis. The key of the correct diagnosis was the history of the patient and the ultrasonography followed by FNAC.