
|
|
Graves' disease - Case 12.
|
|





Clinical data: a 65-year-old woman was referred for evaluation of typical complaints suggesting hyperthyroidism. She was operated on nodular goiter for 19 years. Bilateral subtotal thyroidectomy was performed and histopathology disclosed benign hyperplastic nodules. She never got thyroid medication.
Palpation: both thyroids were enlarged and moderately firm.
Results of blood tests: hyperthyroidism (TSH undetectable, FT4 62.9 pM/L).
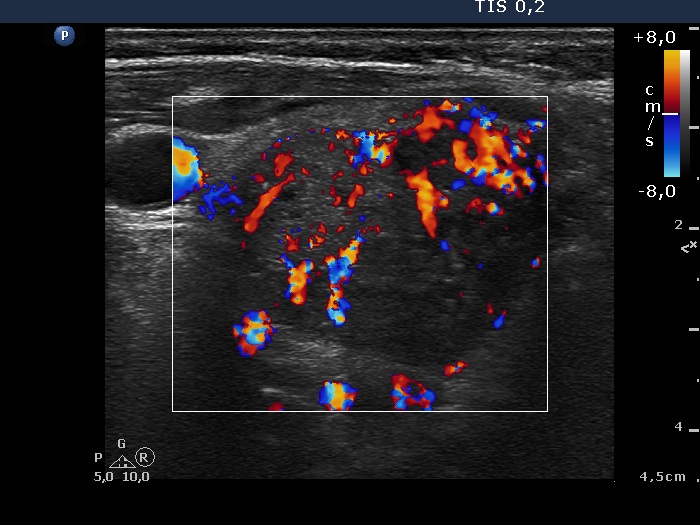
Ultrasonography: both thyroids were diffusely enlarged and were composed of hypoechogenic areas. The vascularization was increased.
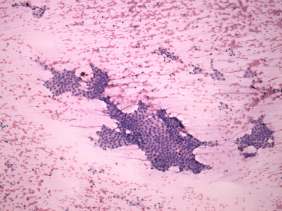
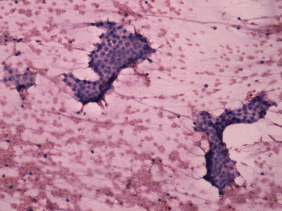
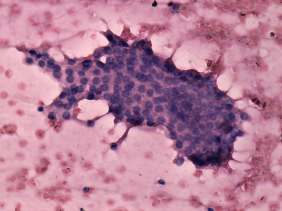
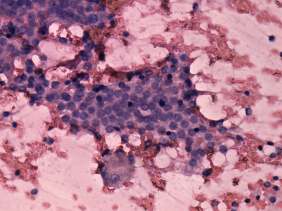
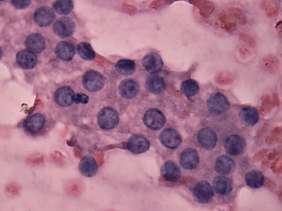
Cytology was performed from the largest hypoechogenic lesion found in the left thyroid. Cytological diagnosis: benign pattern corresponding to hyperthyroidism.
TsAB was elevated 12.1 U/mL (normal value below 1.5) while scintigraphy excluded the possibility of autonomy.
We administered daily 30 mg methimazole. 5 weeks later the patient became euthyroid and we offered radioiodine therapy, but instead of our suggestion, she wanted to be operated on.
Histopathology: diffuse goiter in both lobes and benign hyperplastic nodules in the left thyroid.
Comments.
-
The sonographic pattern of the right lobe is noteworthy and very edifying
-
A hypoechogenic central part is surrounded with an echonormal rim. This pattern mimics that of a large hypoechogenic nodule. Nevertheless, in contrast with a nodular goiter the borders between the hypoechogenic and echonormal fields are irregular, puzzle-like. This pattern is frequently observed in an operated thyroid.
-
The hypoechogenic part of the thyroid is composed of multiple discrete hypoechogenic areas. The retraction between the hypoechogenic fields is probably an artifact and caused by the surgical procedure.
-
-
Patients not infrequently have fear from radioiodine therapy.