
|
|
Graves' disease - Case 11.
|
|















First examination (first and second rows):
Clinical presentation: a 34-year-old woman was referred for an evaluation of a "toxic multinodular goiter". She had typical complaints suggesting hyperthyroidism for 2 months.
Palpation: no abnormality.
Functional state: hyperthyroidism with TSH 0.001 mIU/L, FT4 31.0 pM/L, TSAb 6.2 U/L (normal value < 1.5).
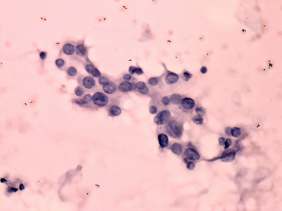
Ultrasonography: the thyroid was echonormal and contained numerous hypoechogenic areas. The echogenicity index was around 25%. The vascularization was moderately increased. Neither of the hypoechogenic areas corresponded to a nodule.Cytology: was performed from the largest hypoechogenic area in the left thyroid.
Cytological diagnosis: benign, atypia of a hormonal reason.
Clinical diagnosis: hyperthyroidism caused by Graves-Basedow disease.
We administered daily 20 mg methimazole to the patient.
5 weeks after the first visit (third row):
Clinical presentation: the patient was well, her complaints had resolved.
Functional state: subclinical hyperthyroidism with undetectable TSH, FT4 12.5 pM/L.
Ultrasonography: the echogenicity index decreased to 15%. The vascularization also decreased. The lesion aspirated on the first visit significantly decreased in size.
The dose of the methimazole was reduced to daily 10 mg.
Comment. The patient had no nodule. In most cases when a patient was falsely diagnosed as having a nodule, we perform aspiration cytology. This is the only chance to completely resolve the unnecessary anxiety of patients from carcinoma.