
|
|
Lymph nodes in the neck - Case 10.Metastasis of a papillary thyroid carcinoma
|
|





Clinical data: a 44-year-old woman was operated on multinodular goiter. A bilateral total thyroidectomy was performed for 2 years. Histopathology disclosed benign, hyperplastic nodules and a solitary focus of a papillary microcarcinoma in the right lobe with a 6 mm maximal diameter. The patient did not get radioiodine therapy. She came to routine follow-up investigation.
Palpation: a firm lesion was palpated lateral to the right thyroid bed.
Functional state: euthyroidism on daily 125 microgram levo-tiroxine (TSH 2.83 mIU/L)
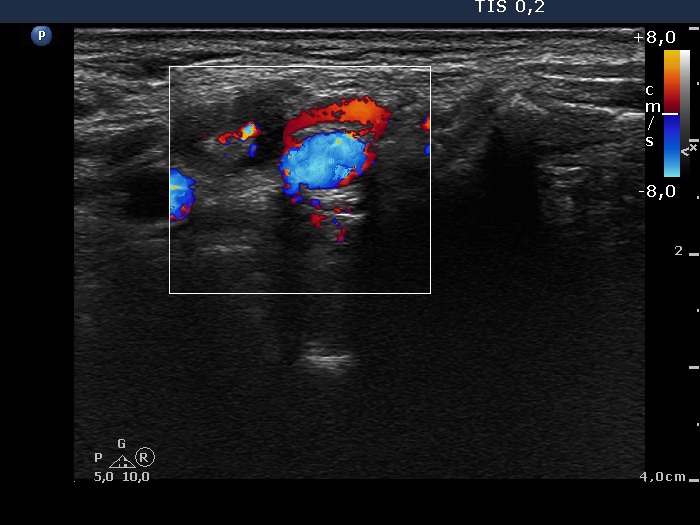
Ultrasonography: there were no thyroid parenchyma in the thyroid beds. A hypoechogenic mass was found lateral to the right lobe. This node presented an irregular hyperechogenic figure.
Cytological diagnosis: benign, reactive type lymph node.
Because of the sonographic presentation we performed thyroglobulin determination from the wash out of the needle which resulted in 38 ng/mL. Serum-thyroglobulin was 3.4 ng/mL.
Modified radical neck dissection of the right lymph nodes was performed.
Histopathology. One of the 11 lymph nodes contained metastasis. The patient underwent on radioiodine therapy.
Comments.
-
This is a relatively rare situation. We do not think that we have to change the management of patients with papillary microcarcinoma on the rare occurrence of metastasis to the lymph nodes in a patient with a classical papillary microcarcinoma, i.e. a solitary focus with less than 10 mm in maximal diameter and no signs of invasion. A solitary papillary carcinoma with the maximal diameter of less then 10 mm does not require radical neck dissection and radioiodine therapy. Nevertheless, these patients have to undergo on regular neck ultrasound examination.
-
This case study emphasizes the importance of the wash-out technique. Ths node contained a small focus of carcinoma and we missed this focus on aspiration. Nevertheless, the elevated thyroglobulin level proved that the needle crossed the focus of carcinoma. A more than 5-fold difference between the wash-out thyroglobulin and serum thyroglobulin levels is an exact proof that the aspirated lesion is of thyroidal origin.