
|
|
Lymph nodes in the neck |
|
Here we discuss only briefly this topic
because we gained experience from a special approach, i.e. by
investigating thyroid patients.
There are several excellent summaries in the literature focusing on the
diagnosis and differential diagnostics of neck lymph nodes.
We offer the article of Dudea et al. and the website of Ying et al.
Why to perform neck ultrasonography?
The neck and the thyroid compose an anatomical unit. We know that the thyroid descends from the tongue during the embryonal period. Therefore, ectopic thyroid tissue with clinical relevance can be found from the tongue to the usual location of the thyroid. This is a very weak argument because ectopic thyroid with clinical relevance is a very infrequent finding and I cannot explain that the routine performance of a neck ultrasound targeting ectopic thyroid would be cost-effective.
Papillary and medullary thyroid carcinomas frequently metastasize to the neck lymph nodes. It means that in patients with thyroid nodules the performance of a neck ultrasound seems to be not superfluous. Nevertheless, the cost effectiveness can be debated.
Irrespectively from thyroid status, patient may harbour disorders presented in the neck. This is again a very weak argument itself. Although we can find by chance a malignant lymph node or a lesion in the salivary gland; these are extremely rare and rare situations, respectively.
Except for nodular goiter patients, the routine performance of neck ultrasound seems to be superfluous. Nevertheless, an experienced sonographer needs an additional one minute or two to scan the neck. Moreover, in the everyday practice we do not waste relevant time: we performed the sonography of the thyroid. Thereafter, we tell the patient what we have found. During this explanation which requires 30 to 90 seconds we can make the sonography of the neck.
Neck ultrasonography in special clinical situations.
Patients after surgery and radioiodine therapy of well-differentiated thyroid carcinoma
Thyroglobulin and anti-hTg are undetectable
This is the situation when neck ultrasound may cause harm. In 10-50% of healthy patients we can find enlarged lymph nodes in the neck. Even theoretically, it seems to be almost unbelievable that an enlarged lymph node could be metastatic in such patients. It is very hard to make believe these patients that the possibility of metastasis can be excluded, therefore great proportion of patients wishes to undergo on FNAC.
Thyroglobulin and/or anti-hTg increased significantly compared with previous examination
The performance of neck ultrasound is mandatory. If we diagnose an enlarged metastatic lymph node by ultrasound and a subsequent aspiration cytology, then surgical procedure would be indicated.
Patients after surgery of medullary carcinoma or oxyphilic variant of thyroid carcinoma
The performance of regular neck ultrasound examination is mandatory. In the former, it is self-evident why to check regularly the patients after surgical therapy. In the case of oxyphilic cell carcinomas, the diagnostic value of thyroglobulin is decreased. Therefore, an undetectable thyroglobulin level does not exclude the possibility of a recurrence.
How to recognize a lymph node?
A lymph node is presented as a
hypoechogenic mass  with
regular, geometrical shape. Most lymph nodes
are oval. A muscle fiber and a vessel may have a similar
appearance,
but both of them are pipe-like. It means that in one axis they may
appear as a node but in the perpendicular section they run along the
transducer. In contrast with the formers a lymph node has an oval shape
in all sections irrespectively of
the angle between the node and the transducer. Therefore, it is
essential to examine a patient in two perpendicular sections.
with
regular, geometrical shape. Most lymph nodes
are oval. A muscle fiber and a vessel may have a similar
appearance,
but both of them are pipe-like. It means that in one axis they may
appear as a node but in the perpendicular section they run along the
transducer. In contrast with the formers a lymph node has an oval shape
in all sections irrespectively of
the angle between the node and the transducer. Therefore, it is
essential to examine a patient in two perpendicular sections.
The use of Doppler mode makes the resolution more easy: we can differentiate a vessel from a lymph node very quickly. On the other hand, Doppler mode is inconvenient to discriminate a thickened muscle fiber from a lymph node.
The differential diagnostics of lymph nodes.
In the everyday practice we can found enlarged lymph nodes in 10 to 30% of patients. Most of them are reactive and has no clinical or oncological significance. A reactive-type lymph node is characterized by the following features:
- a regular hilum,
- a homogeneous or minimally inhomogeneous hypoechogenic structure,
- oval shape,
- sharp borders,
- except for the hilum minimal or no intranodal vascularization and an oval shape.
If a node presents all of these features, the chance of malignancy declines to one-hundredth. Although malignant nodes tend to be larger than benign lymph nodes, the size of a node has a very limited importance in differential diagnostic.
If a lymph node lacks any of the above listed features, we have to palpate the node. A malignant node is only very rarely tender and may be painful only in very advanced cases of a metastatic carcinoma. On the other hand, a bacterially infected lymph node is at least tender in most cases. Such nodes have a blurred borders, round shape, but their hilum is frequently intact. They may contain necrotic or cystic areas.
The role of single features in differential diagnostics.
Lack of a regular hilum
This is one of the two
most important signs of a malignant node. The hilum is the gate of
artery, vein and 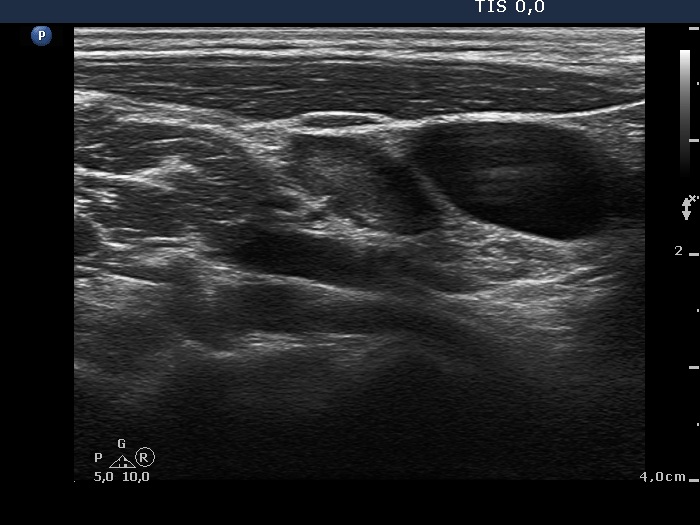 lymphatic
vessel of a node. In the initial phase of a
metastasis, the hilum is already completely intact. In such instances,
the diagnostic value of aspiration cytology is reduced because only a
small part of the node contains malignant cells. In most metastatic
lymph nodes the regular structure of the hilum is disturbed. The hilum
may completely missing or fragmented.
lymphatic
vessel of a node. In the initial phase of a
metastasis, the hilum is already completely intact. In such instances,
the diagnostic value of aspiration cytology is reduced because only a
small part of the node contains malignant cells. In most metastatic
lymph nodes the regular structure of the hilum is disturbed. The hilum
may completely missing or fragmented.
Change in the basic echostructure of the node
 This
is the other one of
the two most important malignant sings. A node containing metastatic
thyroid papillary carcinoma presents frequently cystic fields and
microcalcifications. Metastatic medullary carcinomas frequently display
the characteristic cotton-like patchy hyperechogenic figures. The
presence of necrotic areas is the characteristic feature of metastatic
squamous cell carcinoma. The necrotic foci are irregular echonormal
areas within the hypoechogenic node.
This
is the other one of
the two most important malignant sings. A node containing metastatic
thyroid papillary carcinoma presents frequently cystic fields and
microcalcifications. Metastatic medullary carcinomas frequently display
the characteristic cotton-like patchy hyperechogenic figures. The
presence of necrotic areas is the characteristic feature of metastatic
squamous cell carcinoma. The necrotic foci are irregular echonormal
areas within the hypoechogenic node.
The increased vascularization
 This
is a less sensitive
and specific sign of malignancy than the former properties.
Nevertheless, an irregularly increased
vascularization significantly increases the risk of malignancy. A
papillary carcinoma presenting a type 3 vascular pattern frequently
presents the same pattern when metastatisizing to a lymph node.
This
is a less sensitive
and specific sign of malignancy than the former properties.
Nevertheless, an irregularly increased
vascularization significantly increases the risk of malignancy. A
papillary carcinoma presenting a type 3 vascular pattern frequently
presents the same pattern when metastatisizing to a lymph node.
Blurred and irregular borders of the node
 Blurred
border is a
characteristic sign of a bacterially infected node but it can be seen
even in metastasis of papillary carcinomas. An uneven, irregular,
lobulated shape can be observed
in those malignant nodes where the tumor almost completely
replaces the normal lymphoid tissue.
Blurred
border is a
characteristic sign of a bacterially infected node but it can be seen
even in metastasis of papillary carcinomas. An uneven, irregular,
lobulated shape can be observed
in those malignant nodes where the tumor almost completely
replaces the normal lymphoid tissue.
Wash-out technique in lymph nodes
The technique is the following. We perform a usual fine needle aspiration. After spreading the aspirated material onto the glass we sweep 1 ml 0.9% sodium-chlorid through the needle used for aspiration into the syringe. We rinse the solution in the syringe, thereafter we spout the solution through the needle into the blood collecting glass used for determination of serum thyroglobulin or serum calcitonin, respectively. The subsequent laboratory procedure has to be performed at once and within hours, calcitonin wash-out and thyroglobulin wash-out, respectively.
Thyroglobulin wash-out is a very sensitive and specific
tool in the diagnosis of a metastatic thyroid carcinoma of follicular-cell origin. If the wash-out thyroglobulin exceeds the serum thyroglubulin by 10-fold or more, then the node contained thyroid tissue. If there is no thyroid tissue present in the lymph node, then the wash-out thyroglobulin is usually less than one-tenth of serum level. In our practice only less than 5% of specimens were in the grey zone, i.e. in the range between less than 1/10 to more than 10-fold of serum thyroglobulin level.
We have only very
limited experience with wash-out calcitonin technique because the
technique has a minimal role in primary diagnosis. Thereafter most of
our patients are managed in university centers. So in the event of a
recurrence we only rarely meet these patients.