
|
|
QUICK TOUR - Case studies - sample case 1 of 6:Subacute granulomatous de Quervain's thyroiditis - Case 6. |
|








Initial examination (1st and 2nd rows of images):
Clinical presentation: a 50-year-old woman was referred for an evaluation of neck pain localized to the right thyroid and fever.
Palpation: the right thyroid was painful and hard.
Laboratory examination: hyperthyroidism (TSH 0.01 mIU/L, FT4 43.4 pM/L), CRP 18.3 mg/L.
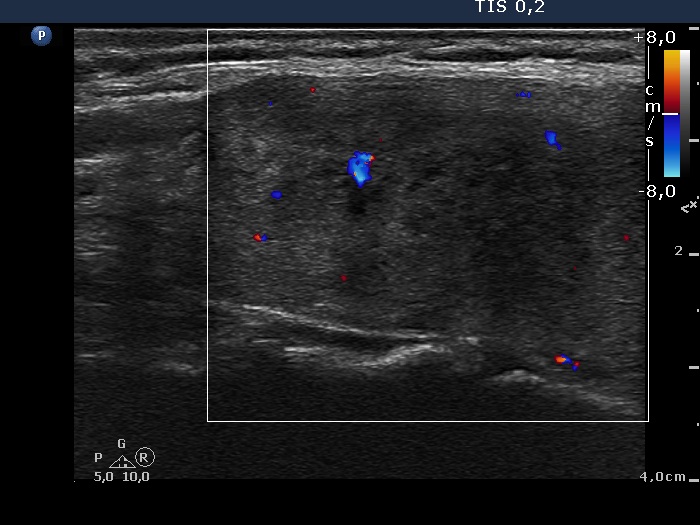
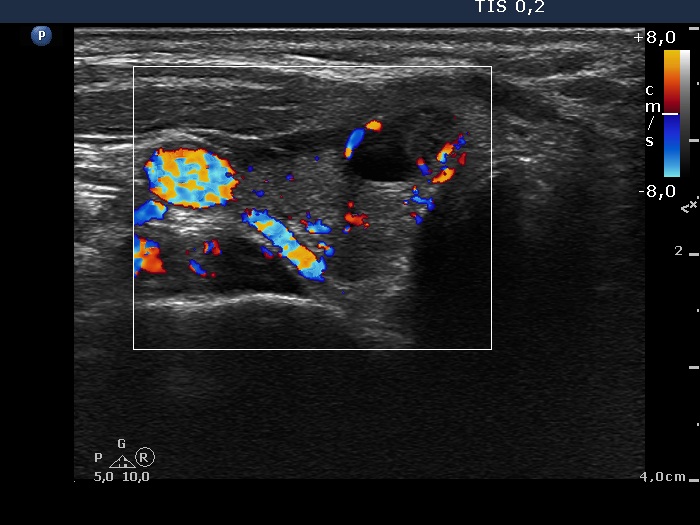
Ultrasonography: there were multiple hypoechogenic areas with ill-defined borders in both lobes, primarily in the right one. The vascularization was decreased.
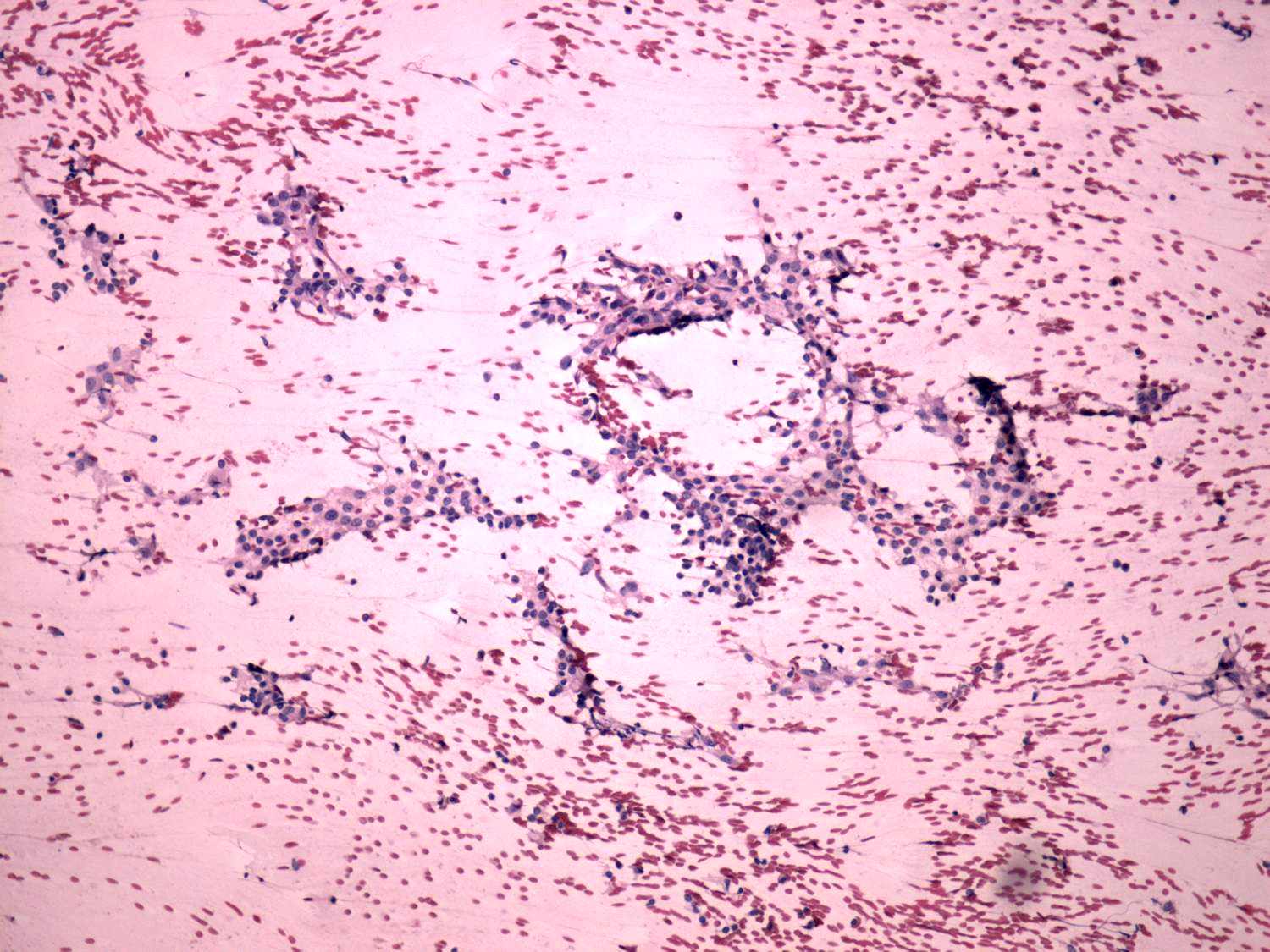
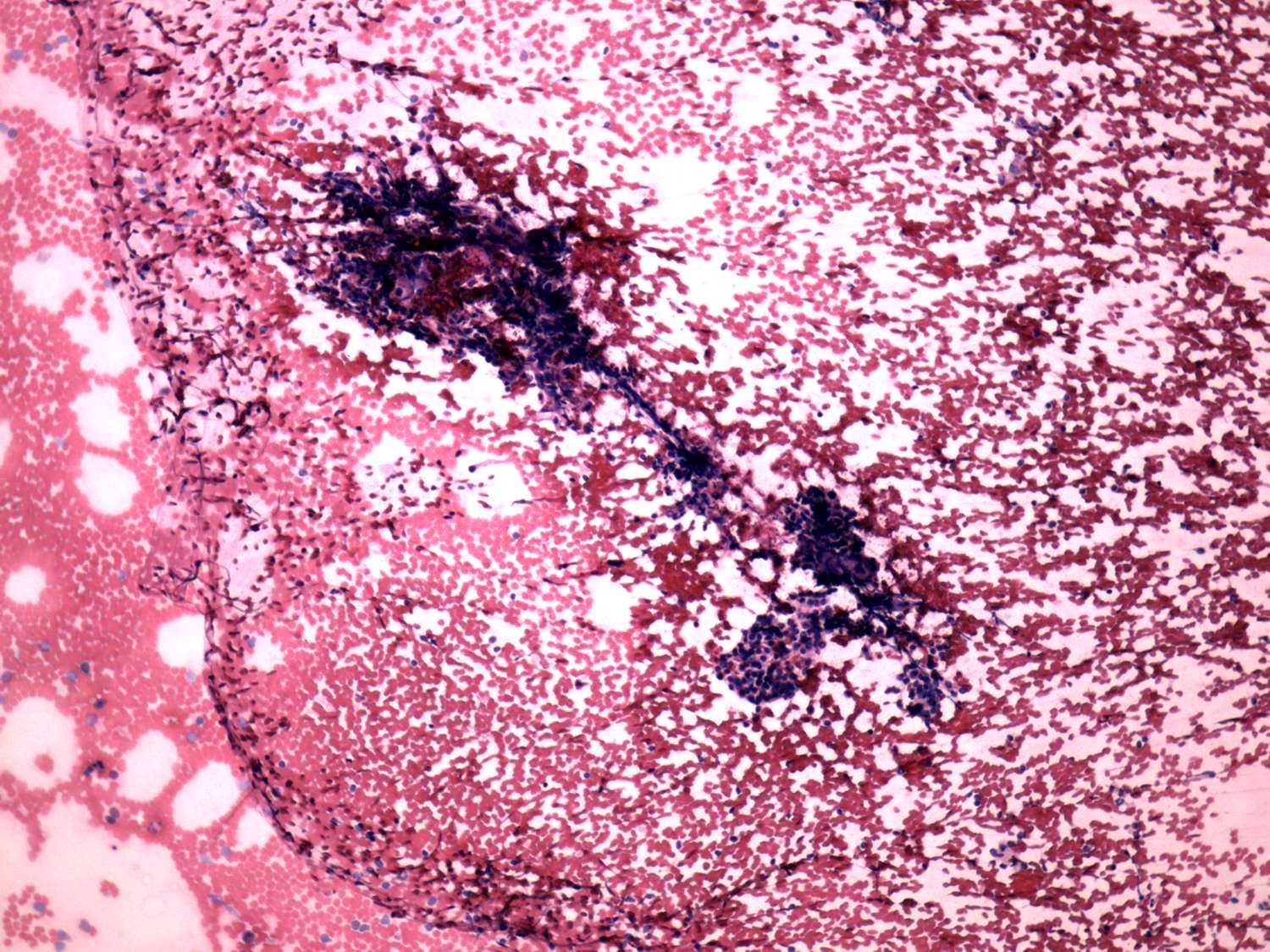
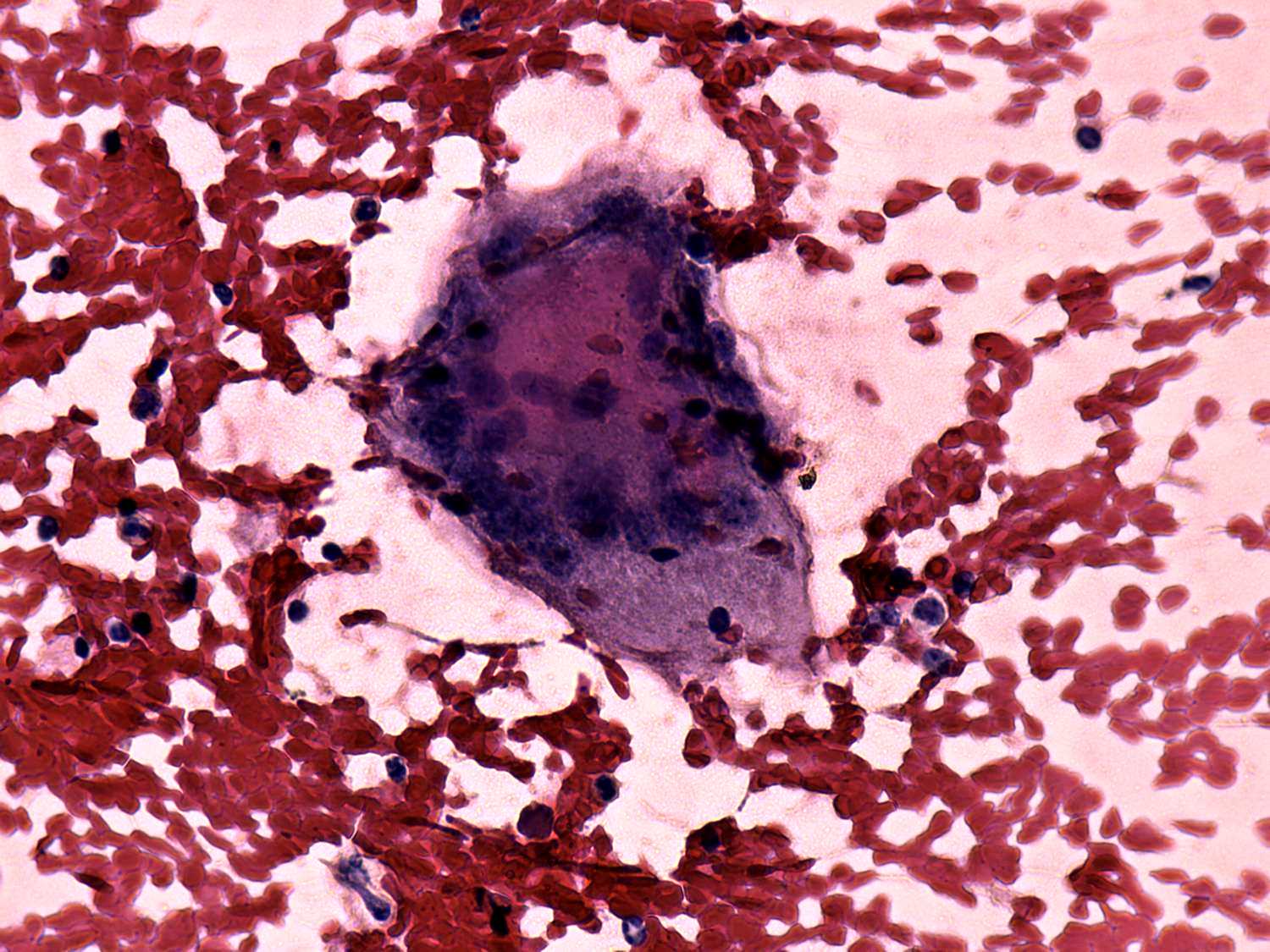
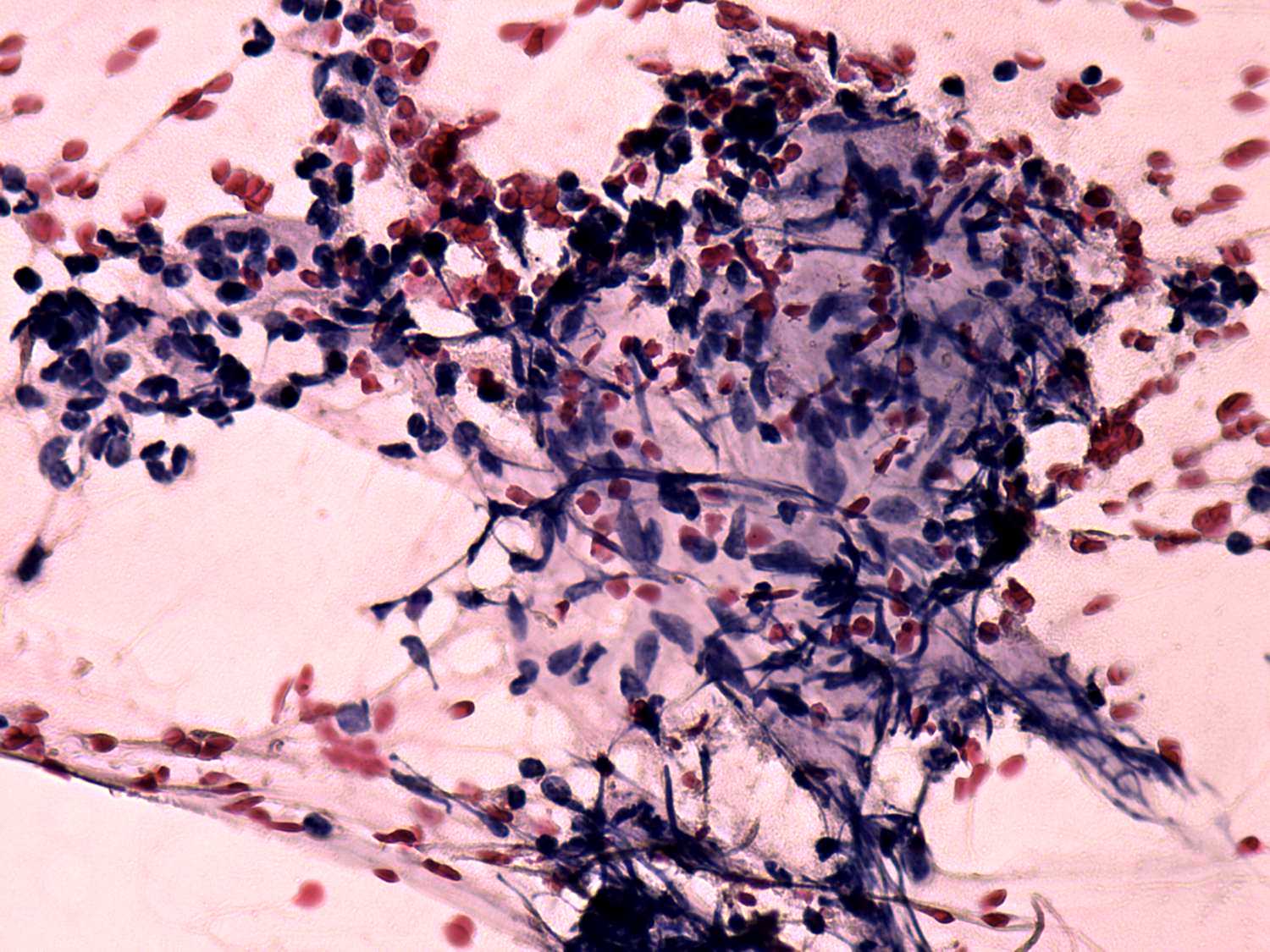
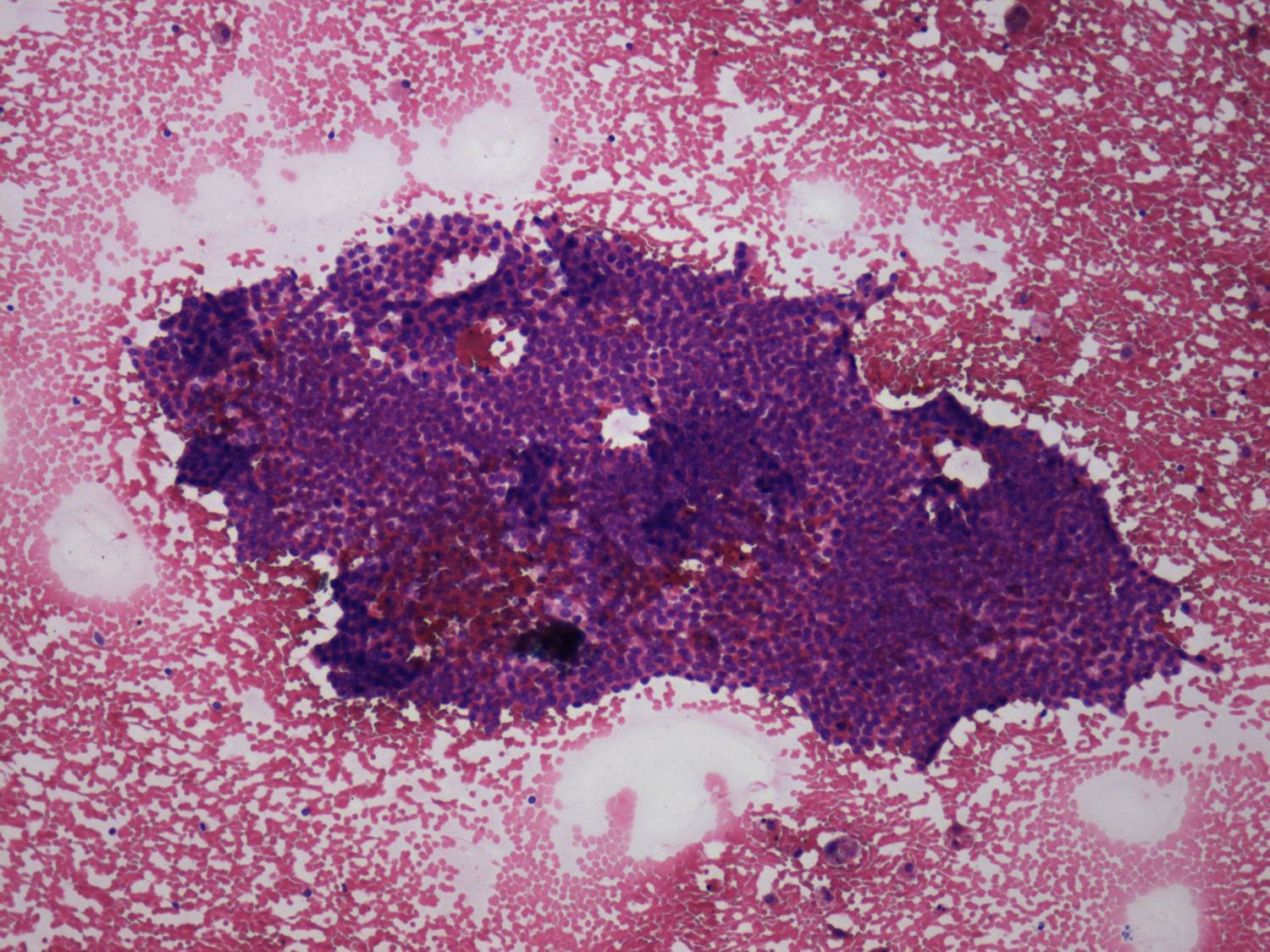
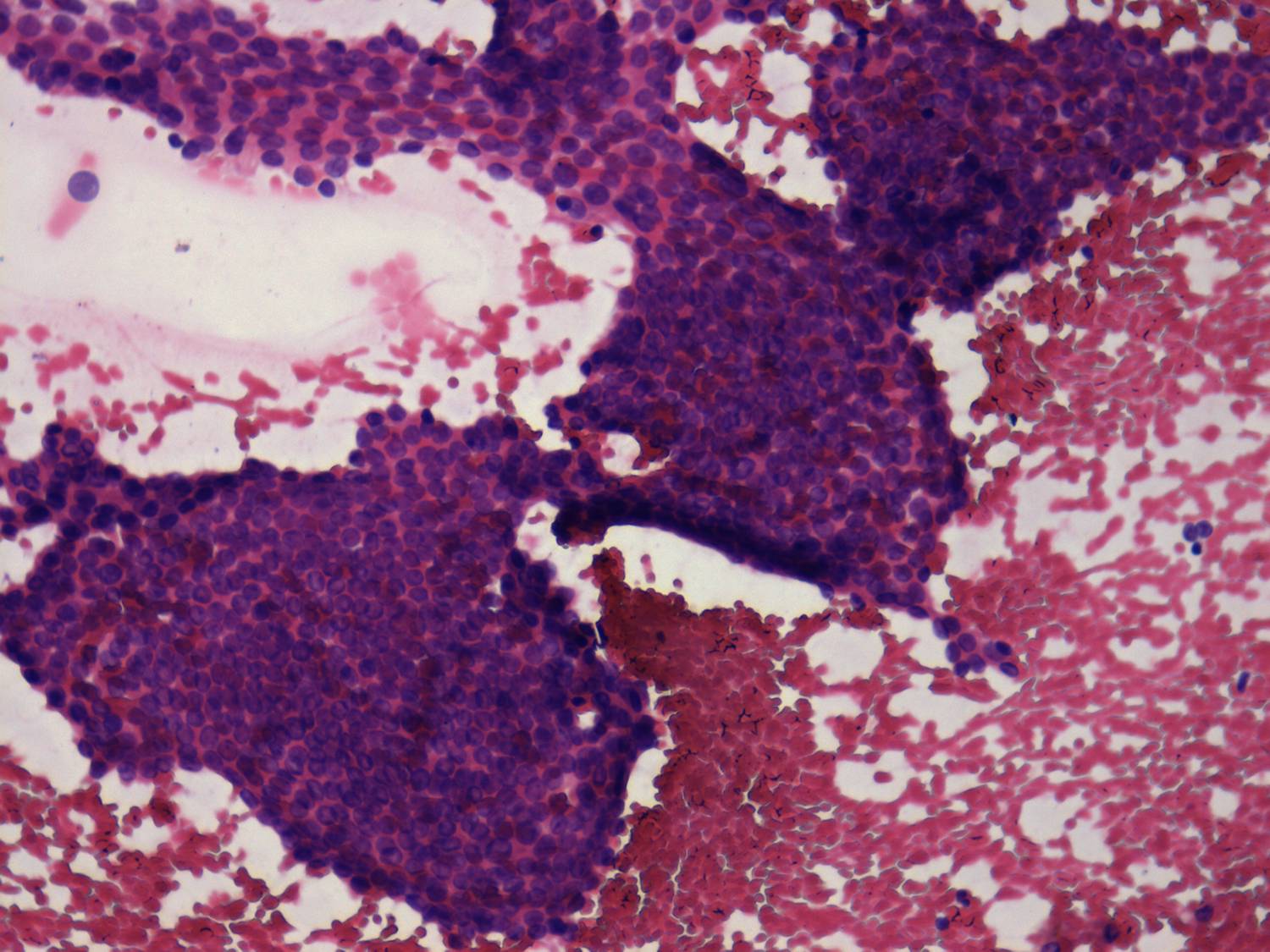
Cytological diagnosis: subacute, granulomatous de Quervain's thyroiditis.
Suggestion: steroid therapy was administered. beta-blocking agent. Within 24 hours of the administration of 32 mg methyl-prednisone, the neck complaints and subfebrility had stopped.
Examination 5 months later (3rd row of images):
Clinical presentation: within 24 hours of the administration of 32 mg methylprednisolone, the neck complaints and subfebrility had stopped and did not recur.
Palpation: the thyroids were minimally tender.
Laboratory tests: minimal degree of hypothyroidism (TSH 4.08 mIU/L, FT4 11.5 pM/L), CRP 0.7 mg/L.
Ultrasonography: the thyroid decreased in size as did the extent of hypoechogenic areas. The vascularization was unchanged. There was a cystic lesion presenting microcalcification in the solid part in the lower part of the right lobe. We reviewed the video of the first examination and noticed that the lesion was already present but much smaller. The difference in size was explained by the lack at cystic component at first investigation.
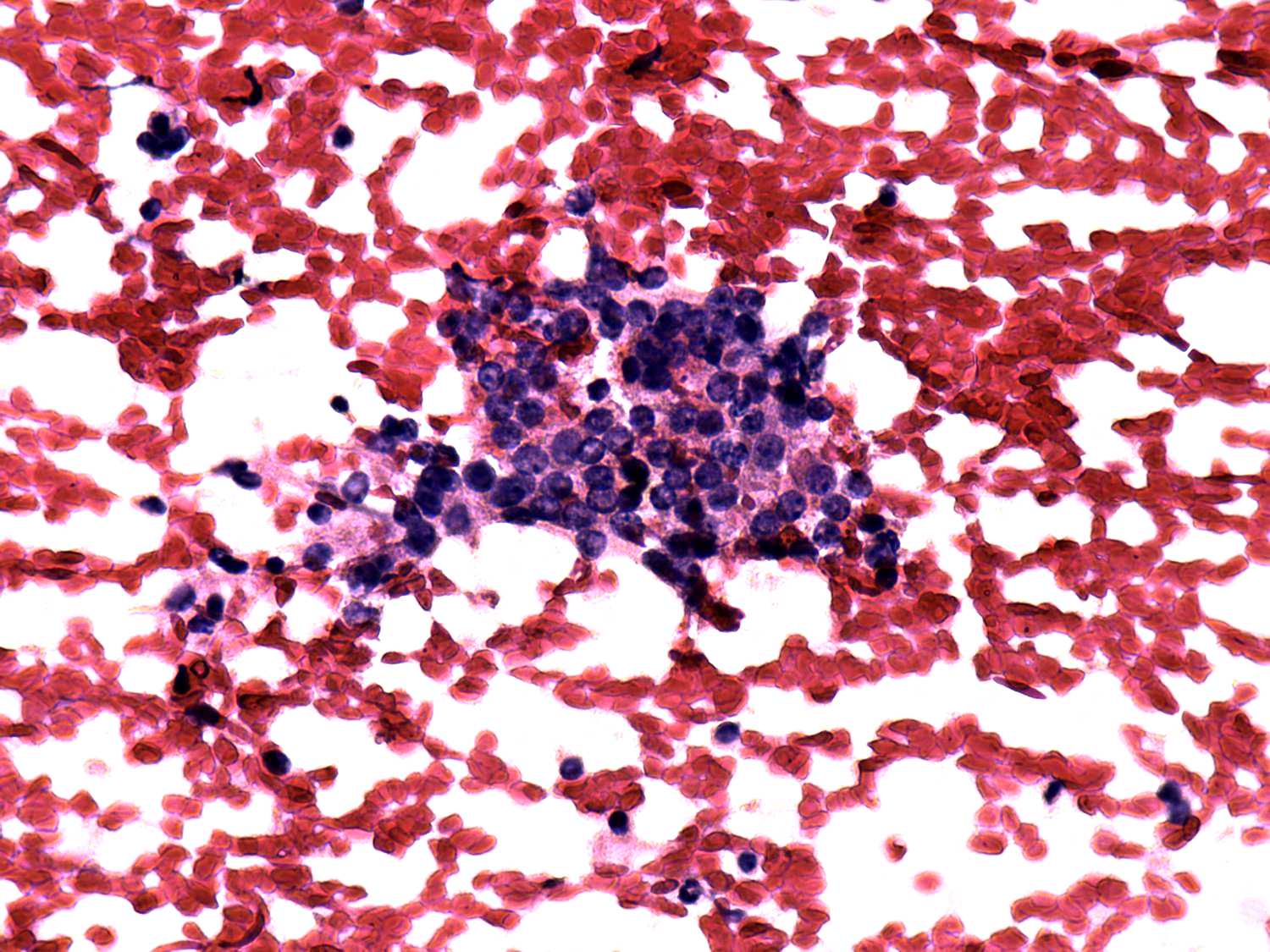
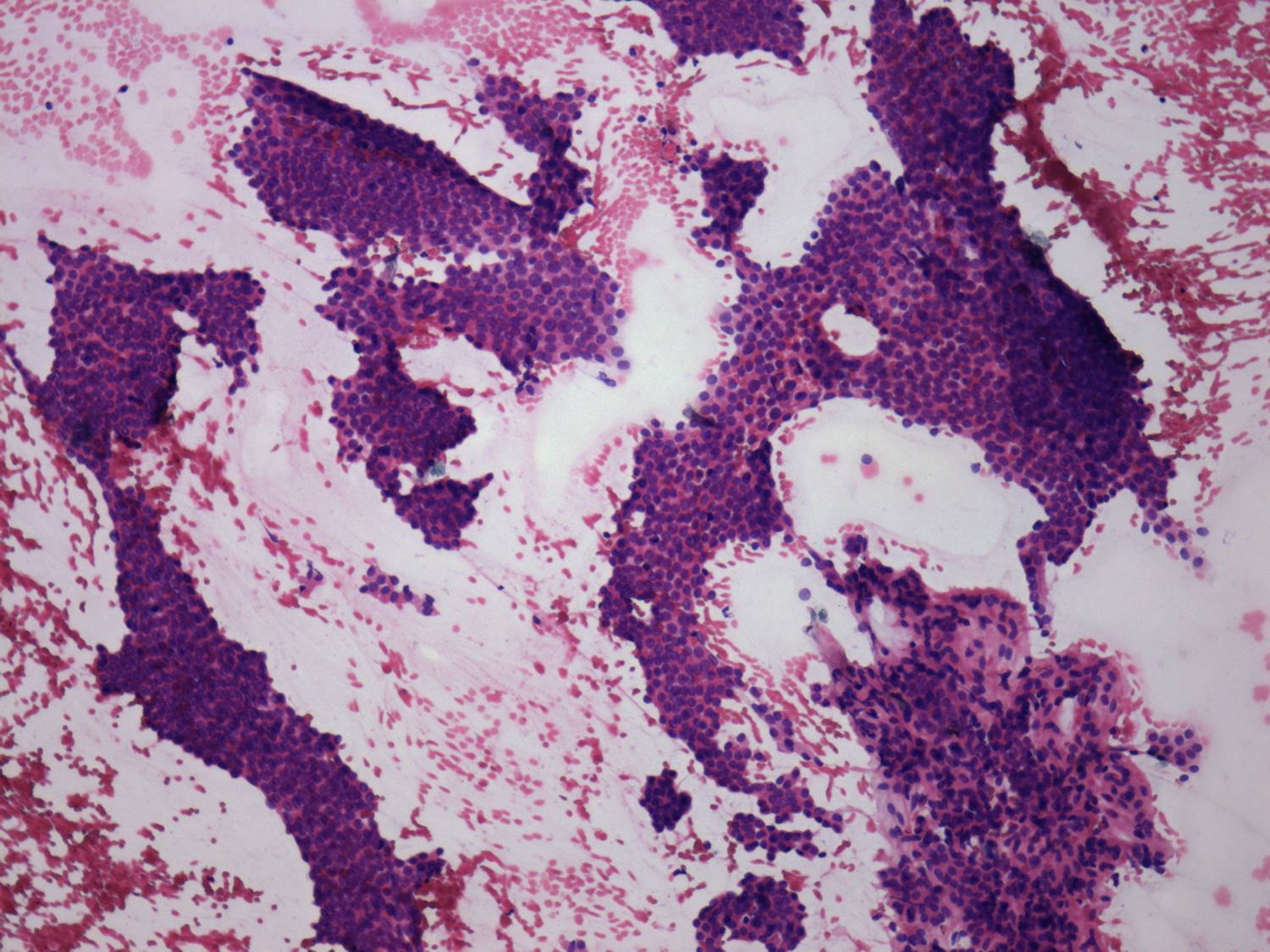
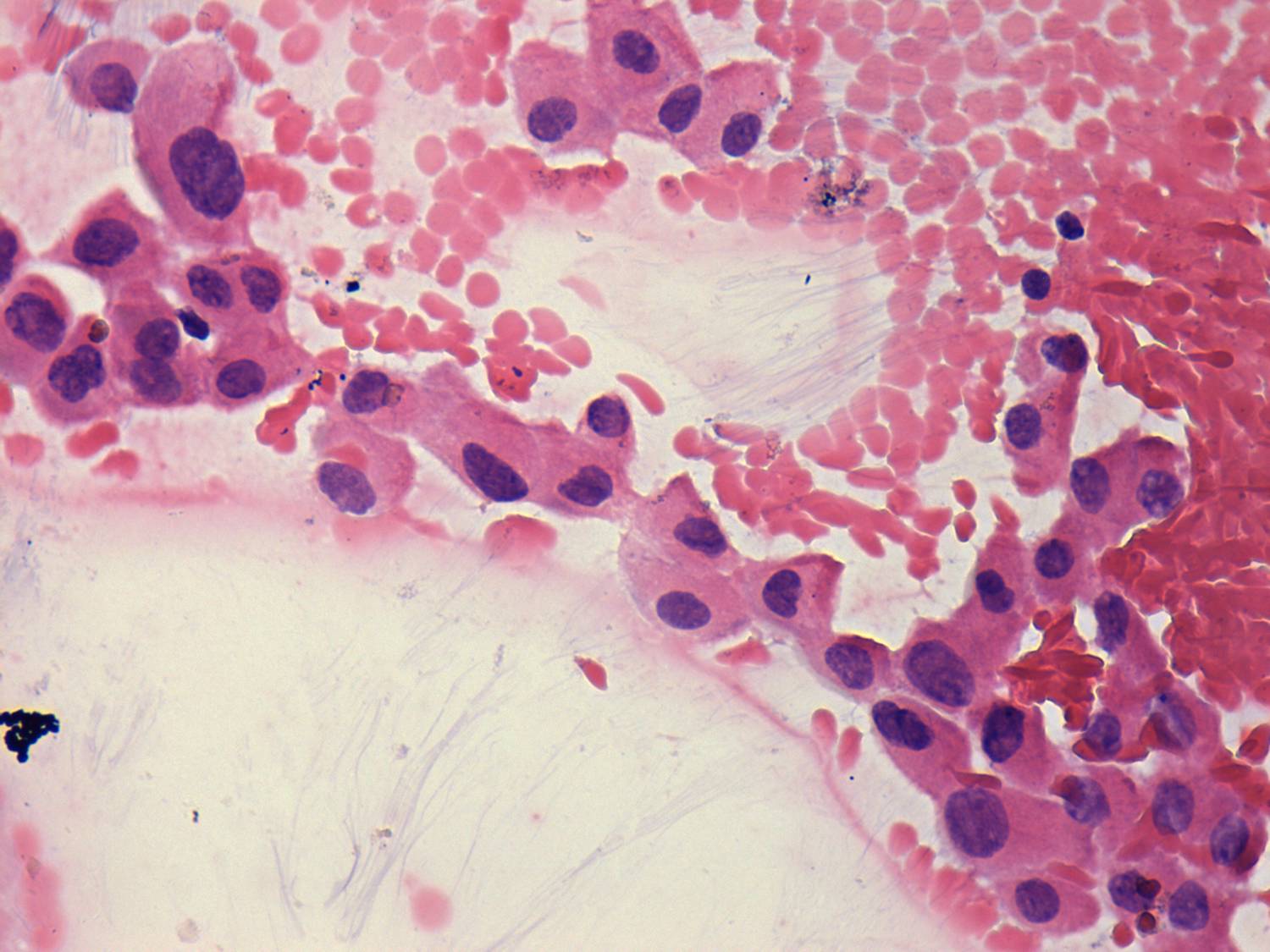
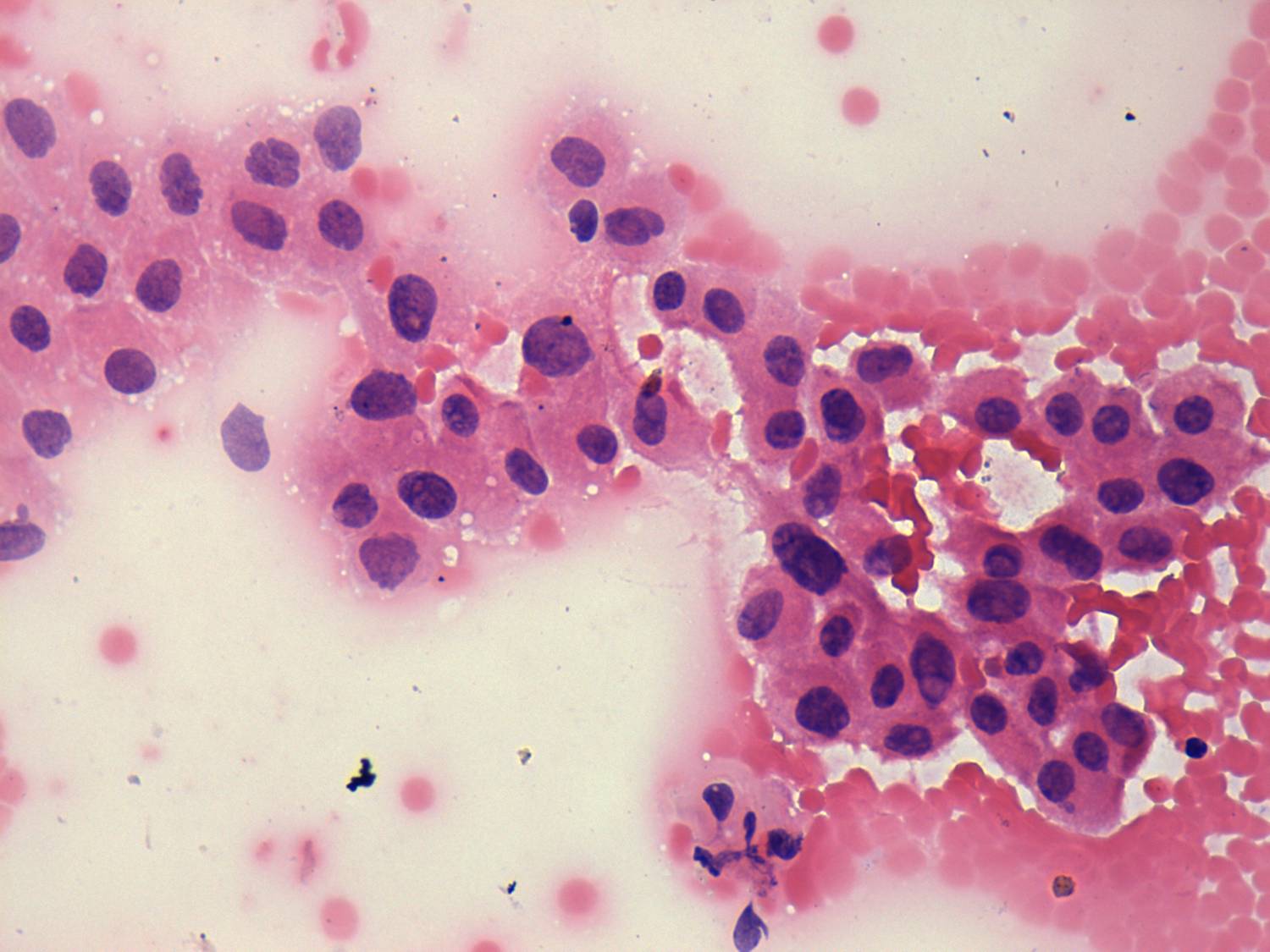
Cytology from the cystic lesion in the right lobe resulted in papillary carcinoma.
Total thyroidectomy was performed. Histopathology discloses a papillary carcinoma. It was solitary with a 4 mm maximal diameter. The left lobe displayed no abnormality.
Comment. Sometimes it is better to overlook a lesion than to recognize it...