
|
|
Thyroid cancers - case 528
|
|



Clinical data: A 64-year-old man was referred for evaluation of a rapidly increasing mass in the left side of the neck. The lesion was first noticed 4 weeks before the present investigation.
Palpation: The left thyroid lobe was extremely enlarged, stone hard.
Functional state: hypothyroidism (TSH 17.1 mIU/L).
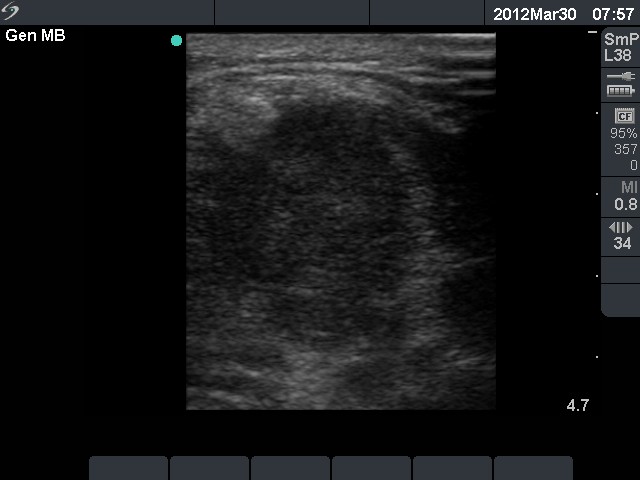
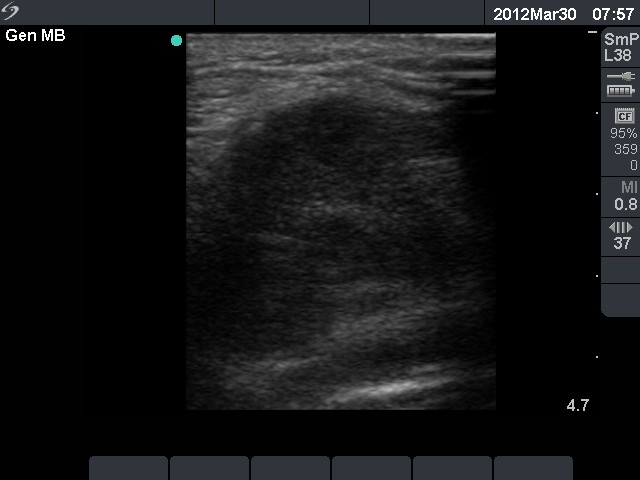
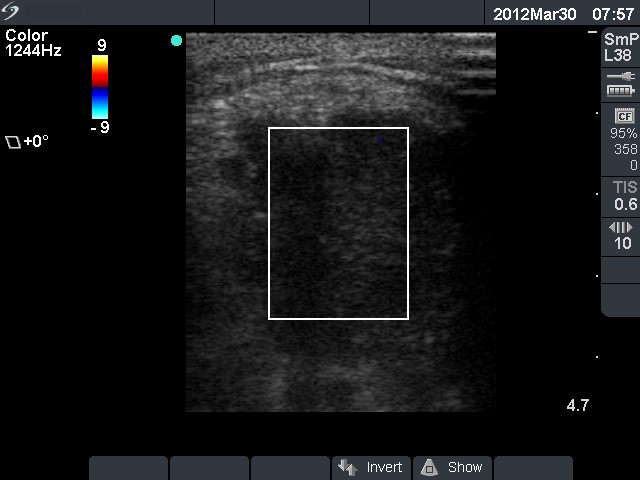
Ultrasonography. The left lobe and the isthmus were infiltrated by multiple hypoechogenic nodules. The transverse diameter of the thyroid was 8 cm, while the longitudinal diameter exceeded 20 cm.
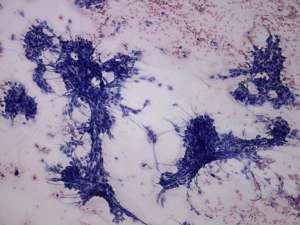
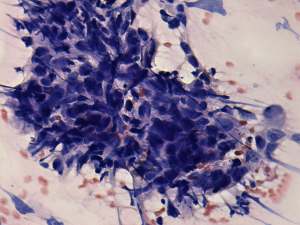
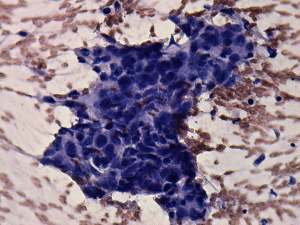
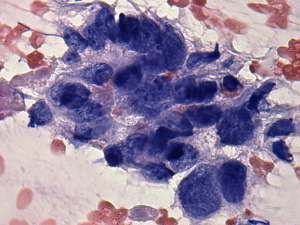
Cytological diagnosis: anaplastic carcinoma.
Histopathology: anaplastic carcinoma.
Comment. The hypothyroidism could cause differential diagnostic problems. The clinical presentation is unequivocal, such tumor must be either anaplastic cancer or MALT-lymphoma. The latter evolves in Hashimoto's thyroiditis and great proportion of the patients have hypothyroidism at the time of diagnosis. Nevertheless, patients with anaplastic cancer may have also hypothyroidism caused by the destruction of the tumor. The frequency of hypothyroidism is around 10-15% in the case of anaplastic cancer. If FNA would not be decisive, the sonographic pattern is be of help: the presence of necrotic foci is a frequent finding in the case of anaplastic cancer but it is a very rare phenomenon in the case of a MALT-type lymphoma.