
|
|
Introduction - case 462
|
|





Clinical presentation: A 17-yr-old boy was referred for evaluation of a nodular goiter. On routine visit at the school doctor, a lymph node was found in the left submandibular area. Thereafter, neck and thyroid ultrasound were performed. On the latter, a hypoechoic nodule was diagnosed in the right lobe.
Palpation: no abnormality in the thyroid. A firm, painless lymph node in the left submandibular region.
Laboratory tests: TSH 3.82 mIU/L, aTPO 0.5 U/mL.
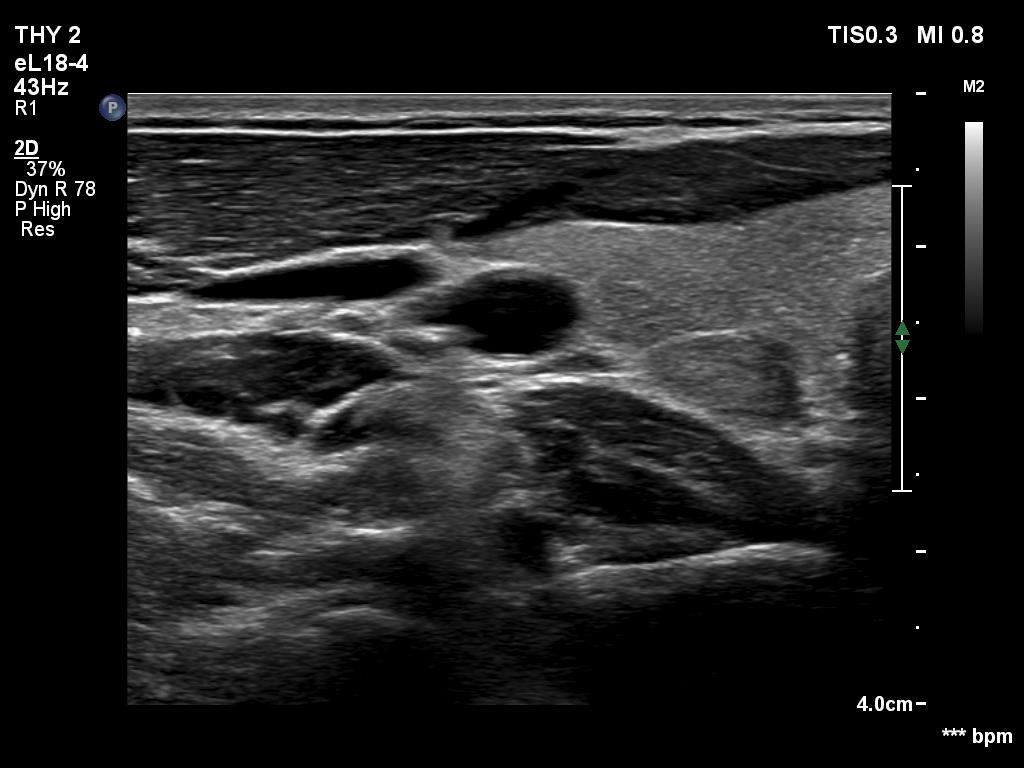
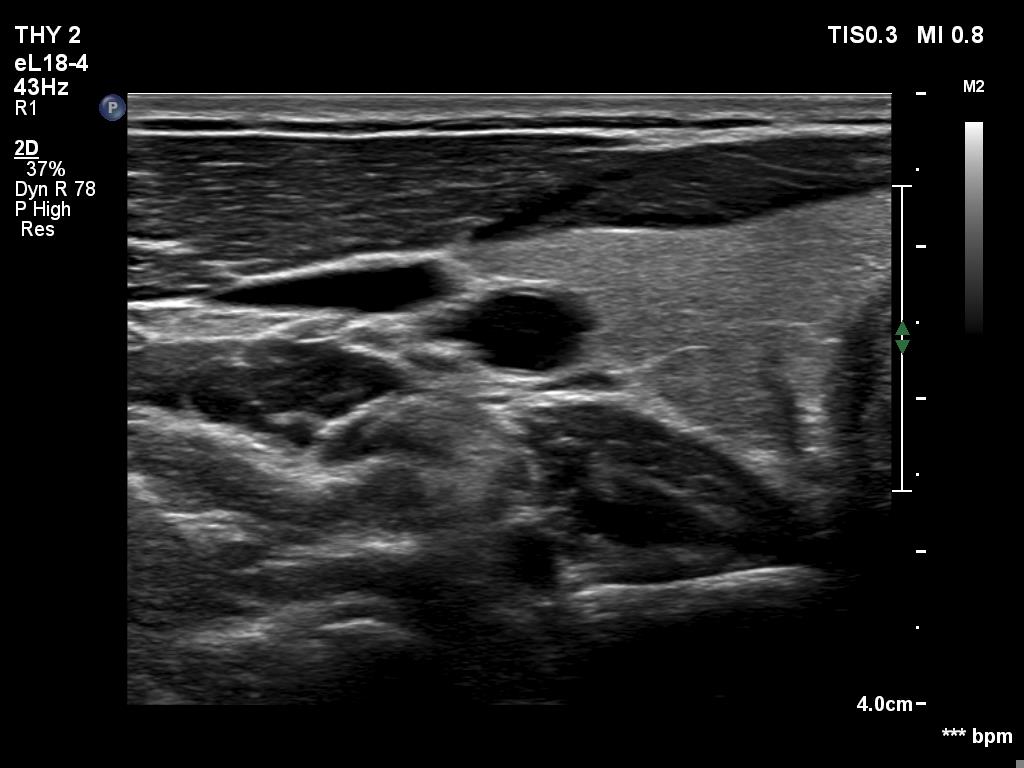
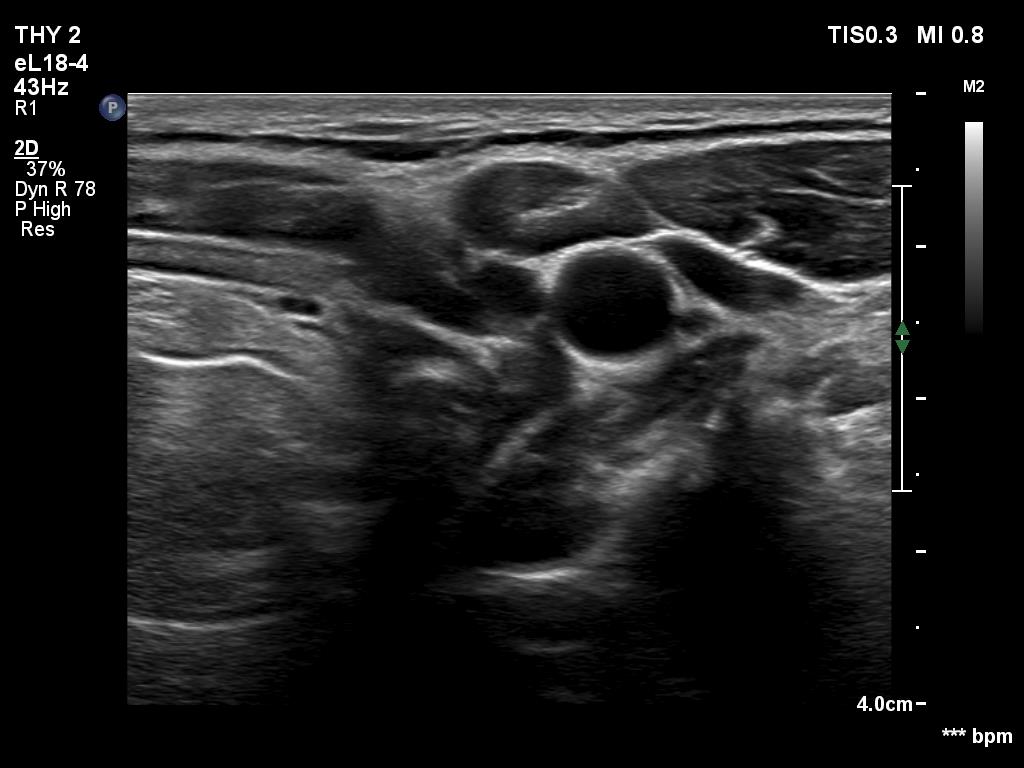
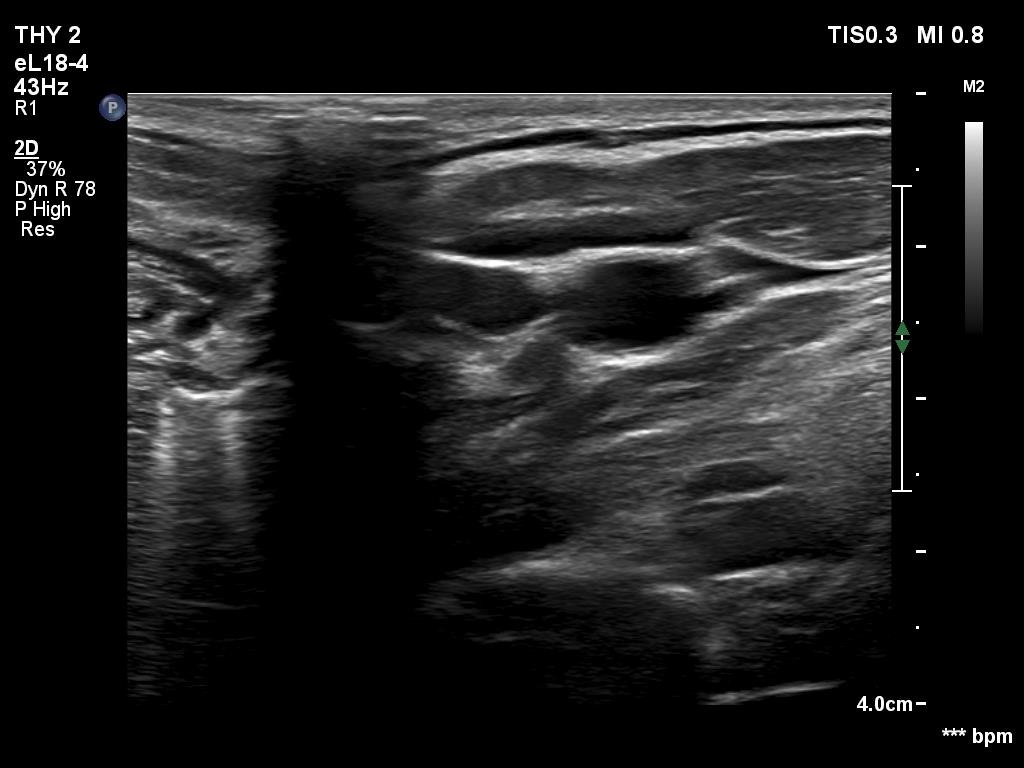
Ultrasonography. The thyroid was echonormal. There was a discrete, minimally hypoechoic area in the dorsal part of the right lobe. This was a technical artifact, caused by a connective tissue band crossing the thyroid. Although on transverse scan, the lesion looked deceptively as a discrete lesion, the real situation became clear on longitudinal scan.
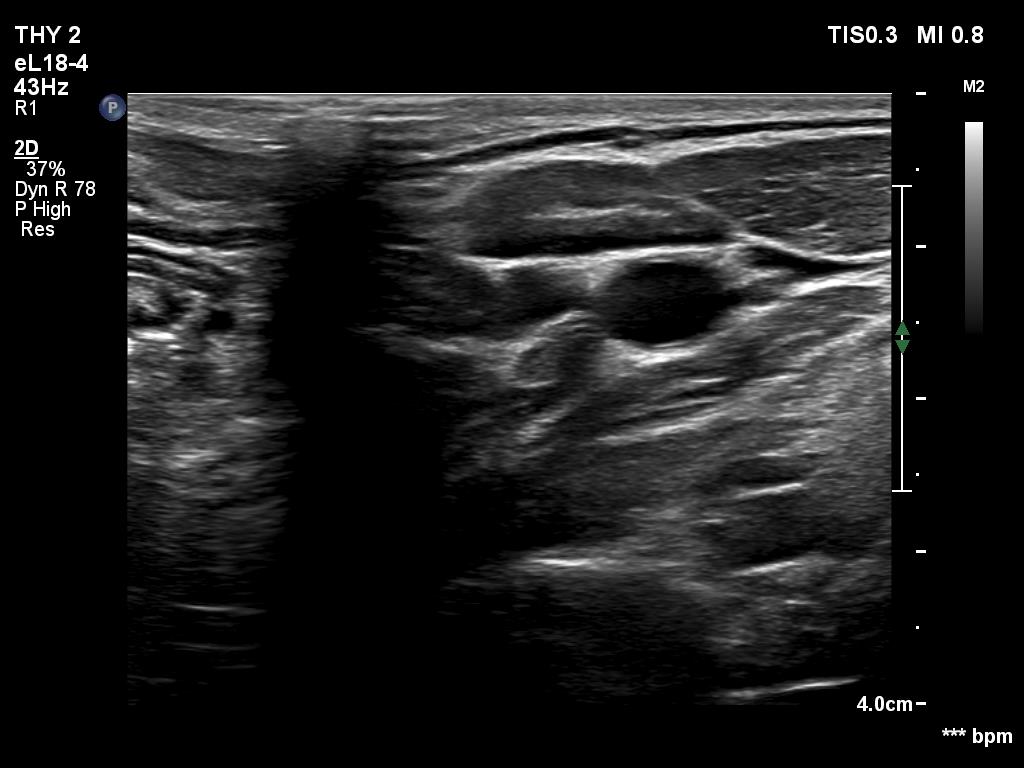
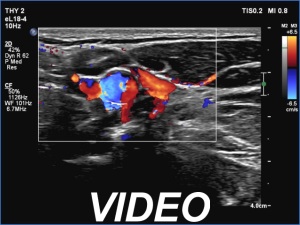
There was a hypoechoic mass with a regular hilum in the left submandibular area. The echo pattern was identical to the neighboring muscle fiber.
Comments.
-
The area in question did not correspond to a discrete lesion. It seemed to be circumscribed because of the presence of connective tissue running ventral which hindered the penetrance of ultrasound wave, therefore made the dorsal area hypoechoic.
-
The differentiation of a lymph node from a discrete thickening of a muscle fiber can be challenging. If the node in this case would be non-palpable then it would be almost impossible to make this distinction. The echo patterns are identical and hilum-like adipose tissue is a common finding in muscle fibers. The only important ultrasound feature is the presence of vascularity according to the hilum. This was not demonstrated on color Doppler mode but was on microflow imaging.