|
|||||||||||||||
|
Differential diagnostic of
Hashimoto's thyroiditis: nuclear details suggesting papillary cancer
|
|||||||||||||||
|
|||||||||||||||
|
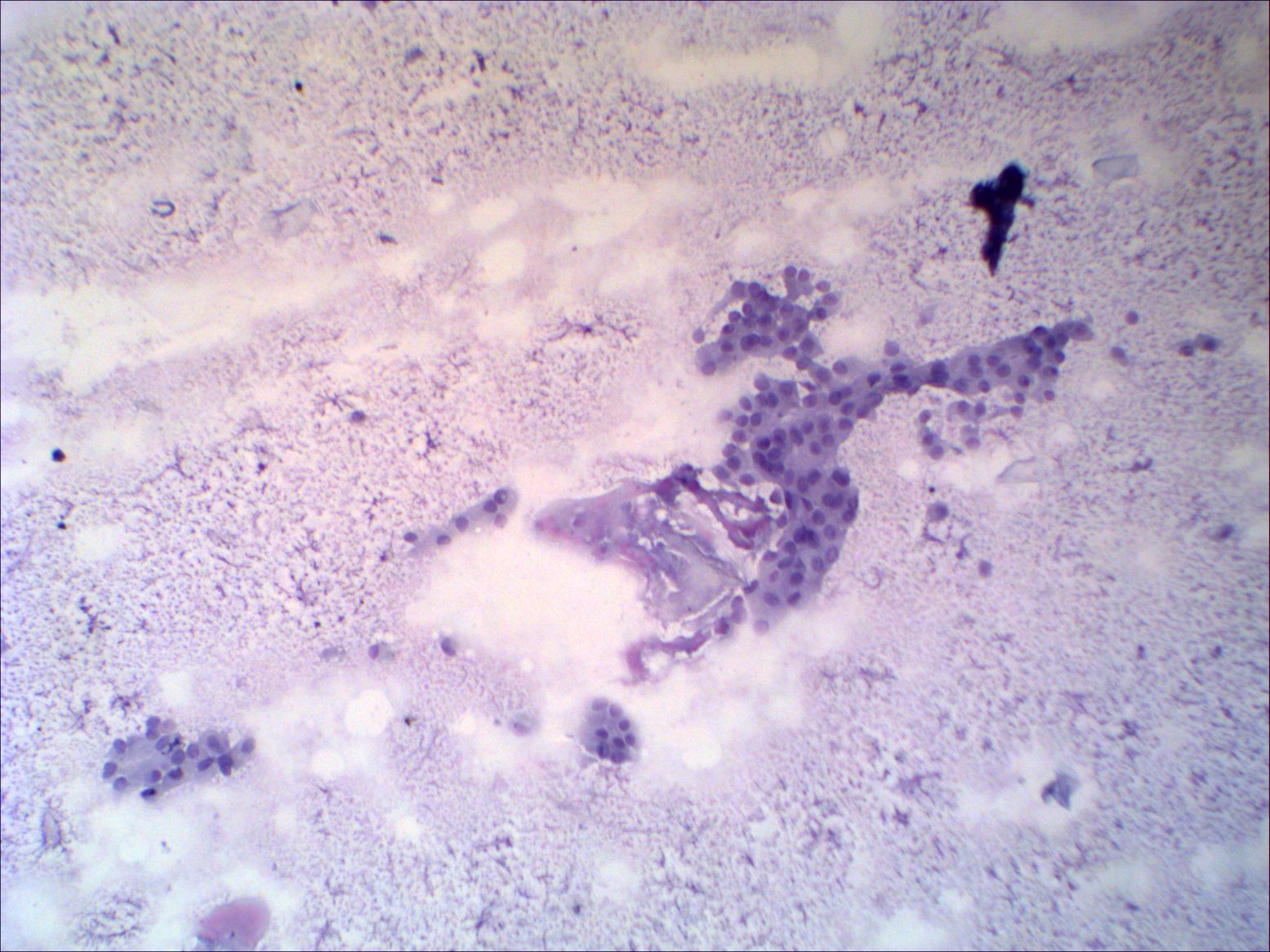
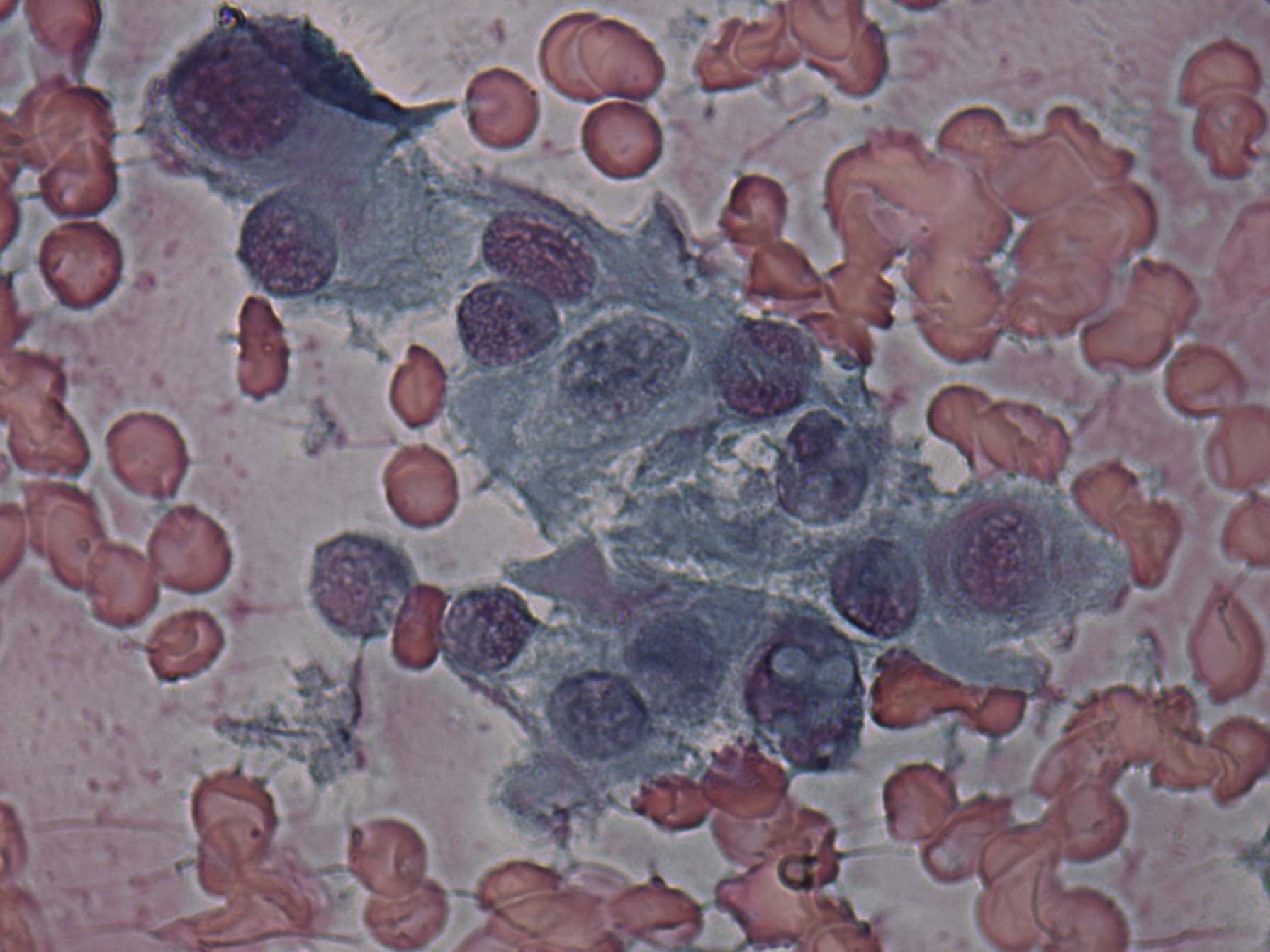
Compare the left
and right images. Histologically verified Hashimoto's thyroiditis is
demonstrated on the left, while histologically proven papillary cancer
on the right. The cytological pattern is again very similar in these
cases. Inclusions which are the most specific sign of papillary cancer
are found even on the left smears, in the case of Hashimoto's
thyroiditis. The presence of lymphocytes within
groups of oxyphilic cells are of greatest help to avoid a false
diagnosis (second images in the left column).
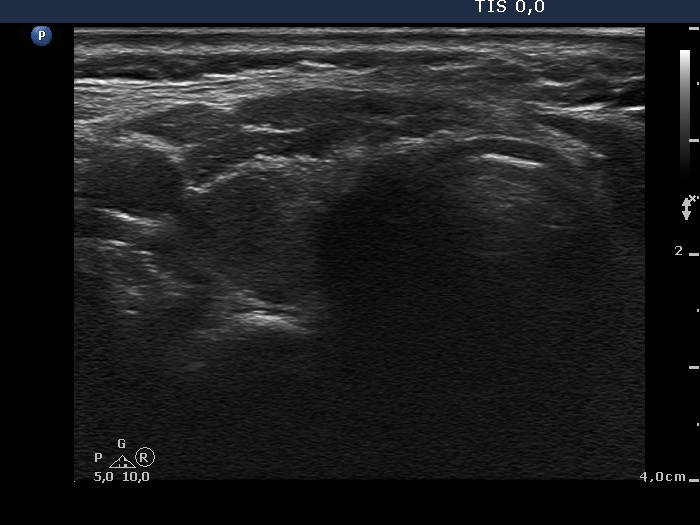
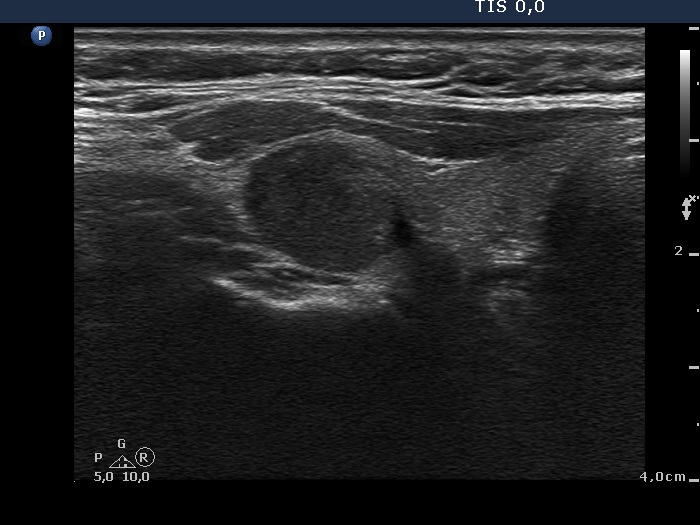
The correct analysis of ultrasound is also not a simple task in neither of these cases. The horizontal view (first ultrasound picture) is equivocal, but the longitudinal scan decides the question. The large hypoechogenic lesion has irregular borders, similarly smaller hypoechogenic areas can be found elsewhere in the lobe, too. Therefore, this lesion is with great probabillity not a nodule in pathological sense. Regarding the ultrasound images of papillary cancer, the pattern highly resembles Hashimoto's thyroiditis. There are several moderately hypoechogenic areas within the lobe. The aspirated one differs from the other lesions because it contains one irregular hyeperchogenic granule. The correct diagnosis in the left, Hashimoto-case was primarily based on the presence of lymphocytes within oxyphilic cell groups and the ultrasound pattern. While in the papillary case the cytologic pattern was decisive: the many intranuclear grooves (second cytologic picture), the papillary structures were the most important cytologic properties leading to the correct diagnosis. The sonographic pattern paradoxically stands against this possibility. |
|||||||||||||||