|
|||||||||||||||
|
Differential diagnostic of
Hashimoto's thyroiditis: nuclear details suggesting papillary cancer
|
|||||||||||||||
|
|||||||||||||||
|
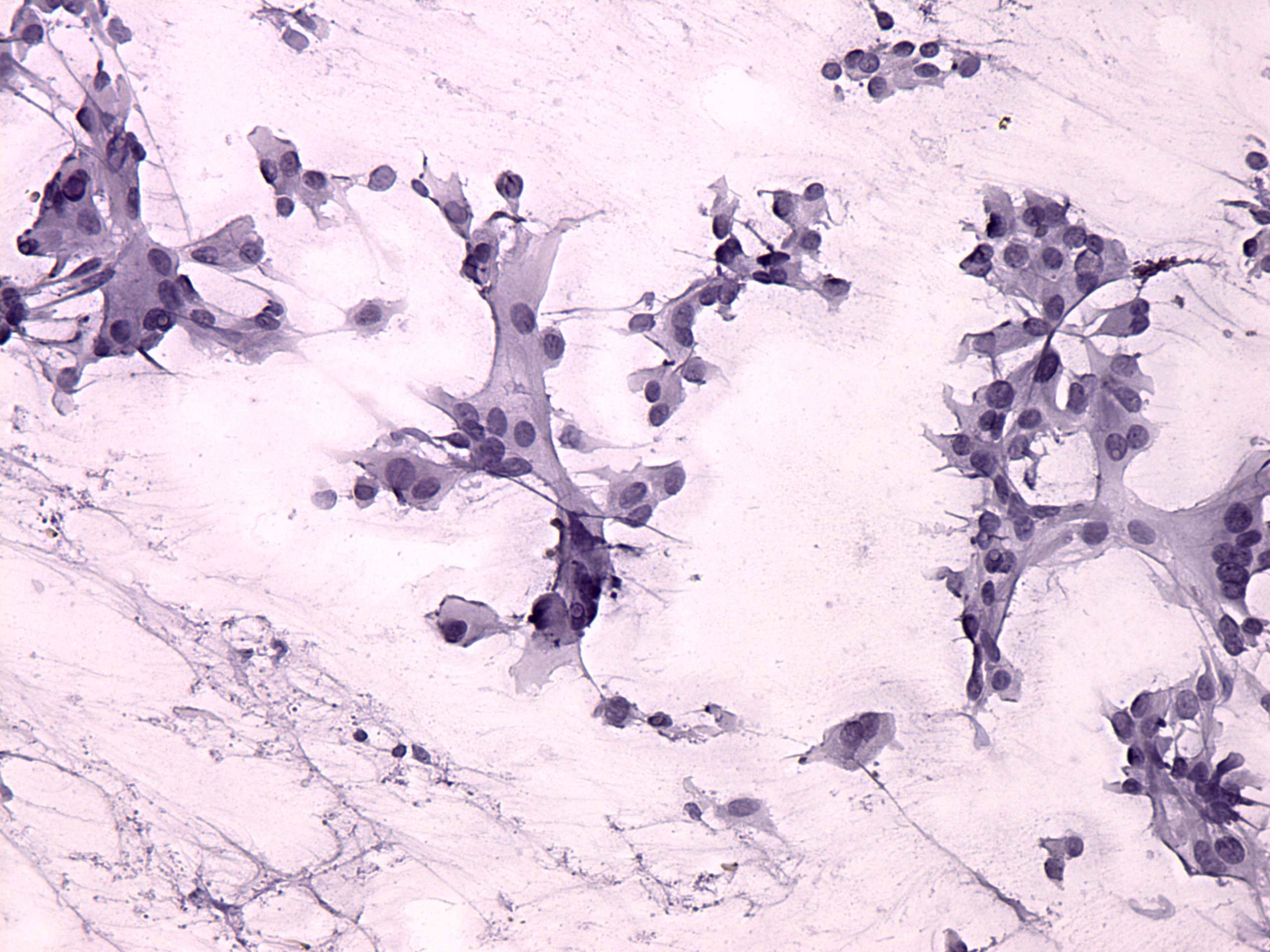
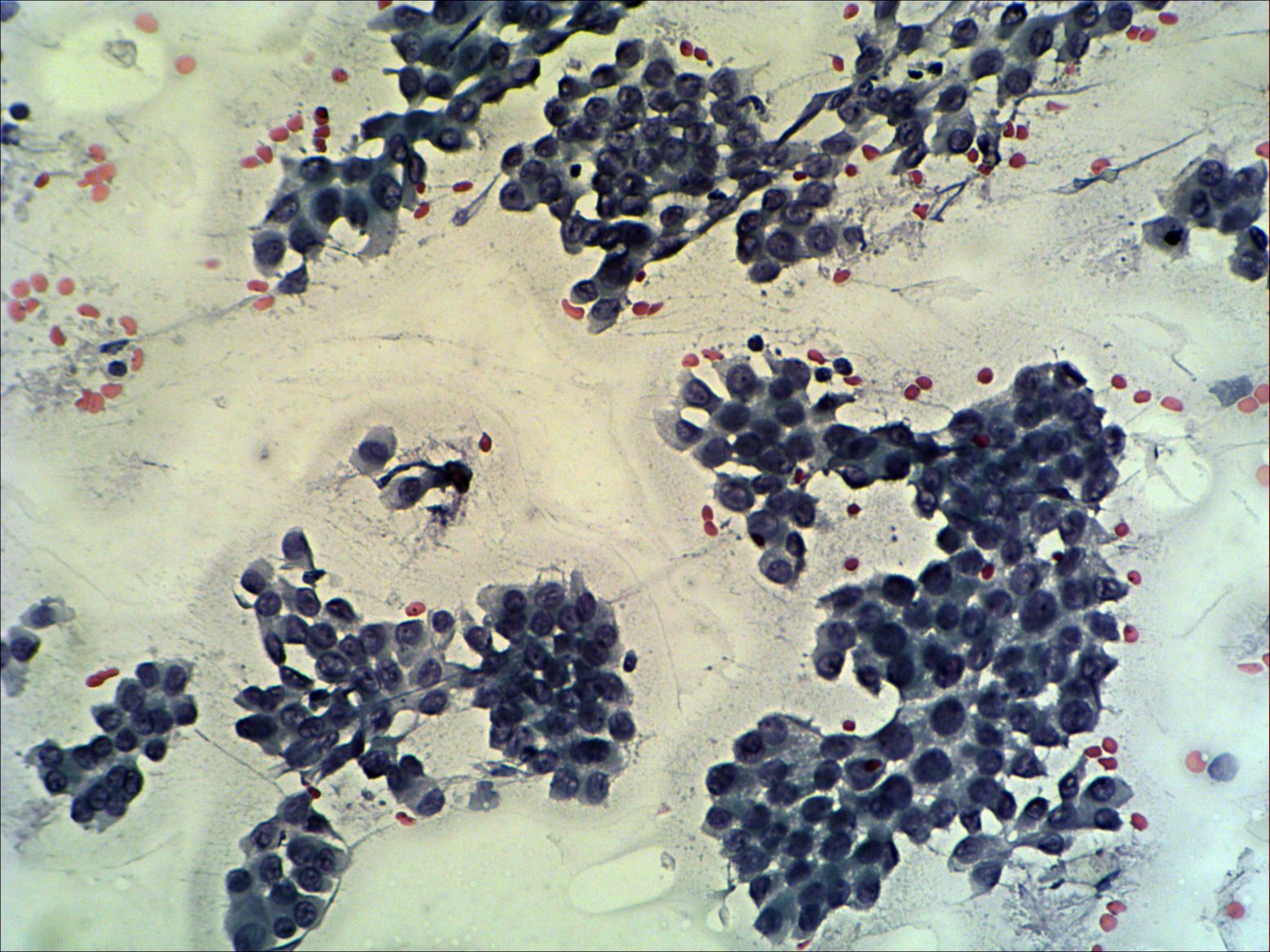
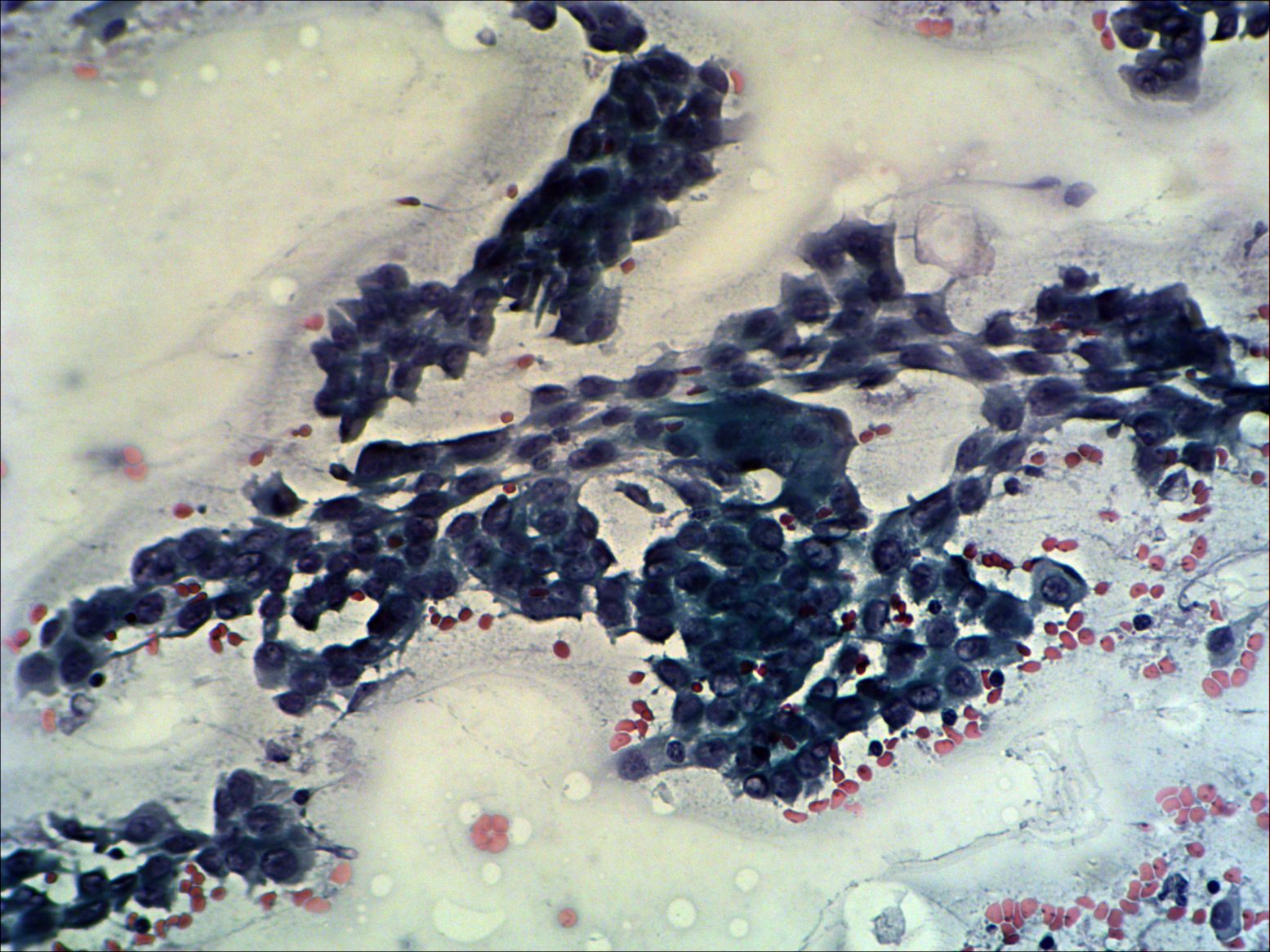
Compare the left
and right images. Histologically verified Hashimoto's thyroiditis is
demonstrated on the left, while histologically proven coexisting
papillary cancer and Hashimoto's thyroiditis on the right. The
cytological pattern is again very similar in these cases. Inclusions
which are the most specific sign of papillary cancer are found even on
the left smears, in the case of Hashimoto's thyroiditis. The presence
of lymphocytes in the second cytologic image and nuclear debris favour
the possibility of thyroiditis. On the other hand, the occurrence of
multinucleated cells is a weak argument which favours the presence of a
tumor.
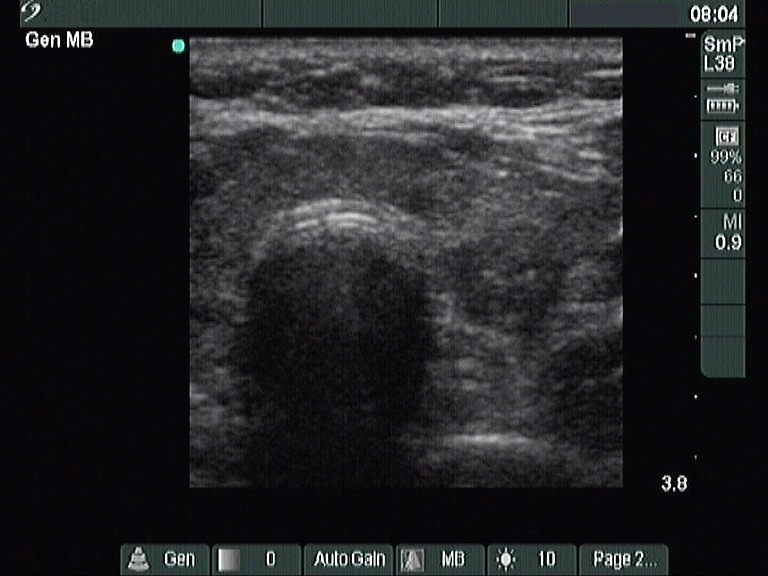
The correct analysis of ultrasound is also not a simple task in the Hashimoto-case. The question is whether the large hypoechogenic area is a nodule surrounded with normal parenchyma or only that part of the lobe which is influenced by thyroiditis. The thorough analysis of the first ultrasonographic picture decides this case. The fibrotic changes within the hypoechogenic area and the puzzle-borders only increase the possibility that this lesion is thyroiditis. The decisive proof can be seen in the ventromedial-isthmic part of the lesion. Unfortunately, we did not record the isthmus and the left lobe, but the hypoechogenic area continued through the isthmus to the left lobe. Therefore it cannot be a nodule. It is worth analysing the sonographic pattern of the papillary cancer on the right, too. The basic echostructure of the thyroid is minimally-moderately hypoechogenic and there are circumscribed moderately hypoechogenic areas within the thyroid. The echostructure of the tumor differs from other parts of the thyroid: it is more hypoechogenic and contains microcalcifications. |
|||||||||||||||