|
 |
 |
 |
 |
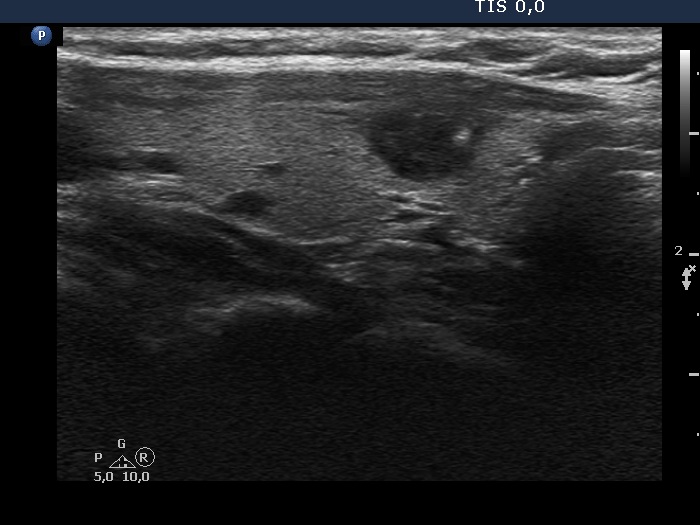
The hypoechogenic part of the nodule has an almost identical echogenicity to the muscle fiber located at the dorsal part of the thyroid. Because the nodule is located at the dorsal border of the lobe, the borders between the nodule and the muscle fiver are indistinctive.
|
| |
|
|
 |
 |
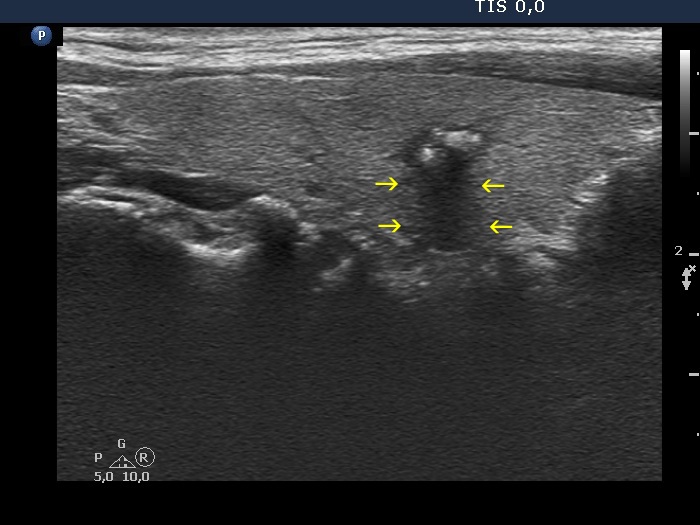
There is a small, less hypoechogenic part in the ventral surface of the nodule (yellow arrow). The echogenicity of this part is identical to that of the muscle fiber running on the ventral border of the thyroid (red arrow). Because the nodule is located in the ventral part of the lobe, these different tissues with identical echogenicity are in contact with each other, which causes a non-pathological blur. On the other hand, the nodule presents pathological blur, as well, this is marked with green arrows.
|
| |
|
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
In this case the thyroid has a large nodule presenting isoechoic areas and the extranodular parenchyma is also isoechoic (yellow arrows). Therefore, a clear distinction is possible in only those parts where halo can be identified in the form of hypoechogenic or hyperechogenic lines between the nodular and non-nodular tissue (red arrows).
|
| |
|
|
Transverse scan
|
Longitudinal scan |
 |
 |
 |
 |
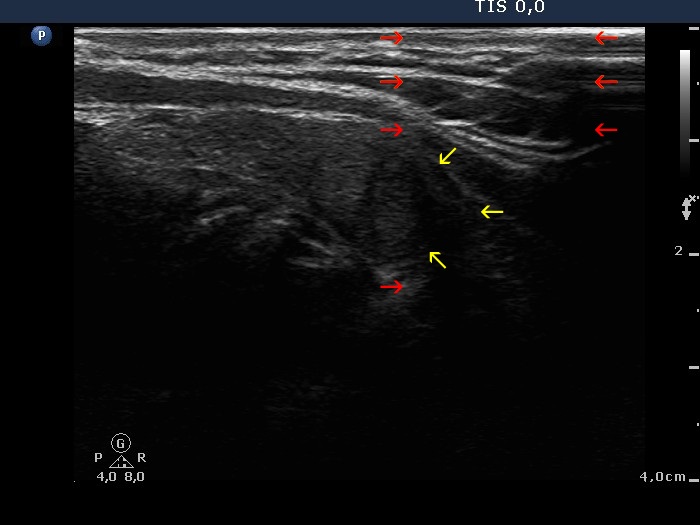
The borders between the nodular area and the non-nodular part of the lobe are indistinctive. The cause of the blur is non-pathological in the ventral part of the nodule (yellow arrows), it can be simply explained by the similar echo structure of the neighboring tissues. On the other hand, the area marked with red arrows should be considered as pathological blur.
|
| |
|
|
|
Transverse scans
|
 |
 |
The region of the dorsal border between the two arrows is suspicious being blurred. On the other hand, the echogenicity of the nodule and the extranodular parenchyma are very similar, therefore it is equivocal whether the area in question should be held abnormal. |
| |
|
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
This is a deceptive pattern. The tumor has macrocalcification, which cannot be visualized. The dorsal acoustic shadow has indistinct borders, but this part of the image (yellow arrows) does not belong to the lesion, this is only an optical artifact. Note that this deeply hypoechogenic band runs deeply dorsal.
|
| |
|
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
The pattern of the transverse scan is very deceptive, the hypoechogenic area (marked with red arrows) dorsal to the less hypoechogenic main body seems to have ill-defined borders. However, if we analyze the longitudinal scan, we can realize that the blurred area (pointed with yellow arrows) dorsal to the main body of the lesion is caused simply by acoustic shadow of a macrocalcification located in the ventral part of the nodule. Note that the acoustic shadow extends beyond the dorsal part of the lobe.
|
| |
|
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
The situation is the same as in the previous case: a dorsal acoustic shadow mimics blurred borders. And again, the extension of the ill-defined part is decisive, it can be followed to the dorsal surface of the thyroid (yellow arrows).
|
| |
|
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
The borders of the nodule are partly indistinctive (yellow arrows). However, note that the hypoechogenic rectangular area, which starts at the most ventral part of the image, extends to the most dorsal part. This is an optical phenomenon caused by the improper fitting of the transducer to the neck of the patient.
|
| |
|
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
Great proportion of the nodule' borders are indistinctive. However, the cause of the blur is very likely not pathological. First, the focus was set wrongly (red arrow), therefore the dorsal part of the nodule is difficult to judge (yellow arrow in the transverse scan). Second, the upper and lower parts of the nodule are blurred (yellow arrows in the longitudinal scan) because of the placement of the transducer. It can be difficult to fit properly the probe all along to the patient's neck.
|
| |
|
|
Transverse scan |
Longitudinal scan |
 |
 |
|
 |
In contrast with the images of transverse scan, where the borders of the nodule seem to be ill-defined, longitudinal scan images present sharp borders. The difference is caused by the placement of the transducer: in the event of transverse scanning the positioning of the probe all along parallel with the neck structures can be more difficult because of anatomical situation. Note that the images differ not only in nodule' borders but in the basic echogenicity, as well.
|
| |
|
Bening colloid goiter - case 2119 |
Wrong settings |
Right settings |
 |
 |
 |
 |
This case illustrates the significance of two issues, an avoidable and an unavoidable cause of non-pathological blur. Regarding the former let's compare the upper images. We can see that both the focus was improper and the general setting was also set incorrectly to 'R' (resolution, i.e., to higher frequency). After proper focusing and proper setting to 'P' (penetration, i.e. to lower frequency), the dorsal blur of the image has disappeared in the right image. On the other hand, the nodule was relatively large and even if the settings are good, we can't make the lower part of the nodule clearly visible.
|
