|
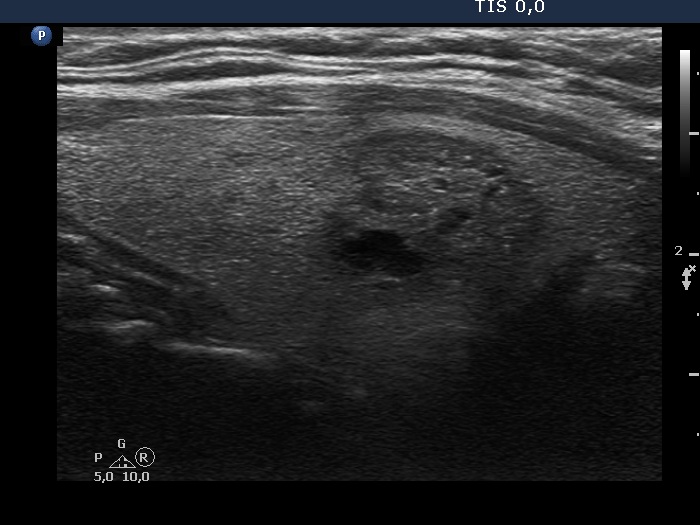
Transverse scan |
Longitudinal scan |
 |
 |
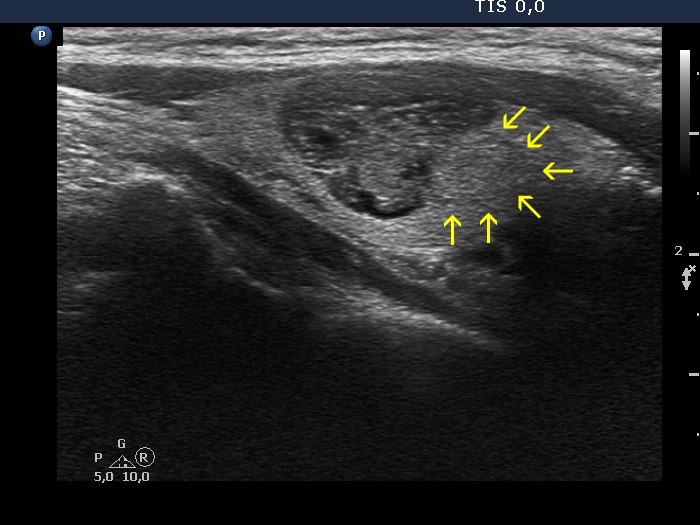
Although the whole nodular area seems to be lobulated, the cause for this lobulated appearance is the complex structure of the area which is composed of three distinct lesions. This pattern should not be judged as lobulated.
|
| |
|
|
Transverse scan |
Longitudinal scan |
 |
 |
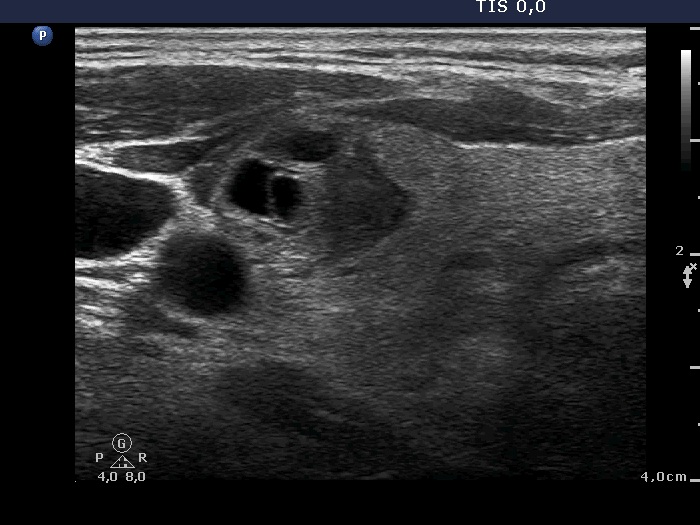
The nodular area is composed of multiple lesions causing a lobulation of the entire mass. As in every case, we should rely on video record to judge whether any of the lesion would have lobulated margins. The video proves that neither of them does.
|
| |
|
|
Transverse scan
|
 |
 |
Longitudinal scan
|
 |
 |
This nodular area has lobulated margins. On the other hand, it is equivocal whether the nodular area is composed of one or more discrete lesions. In the former case this would belong to TIRADS-5 category and would require cytological evaluation. If we consider that there are two or more nodules, than the most suspicious, ventral moderately hypoechogenic nodule is a TIRADS 4 category lesion and FNA would not be indicated based on the ETA TIRADS, because the maximal diameter is less than 15 mm.
|
| |
|
|
 |
 |
 |
 |
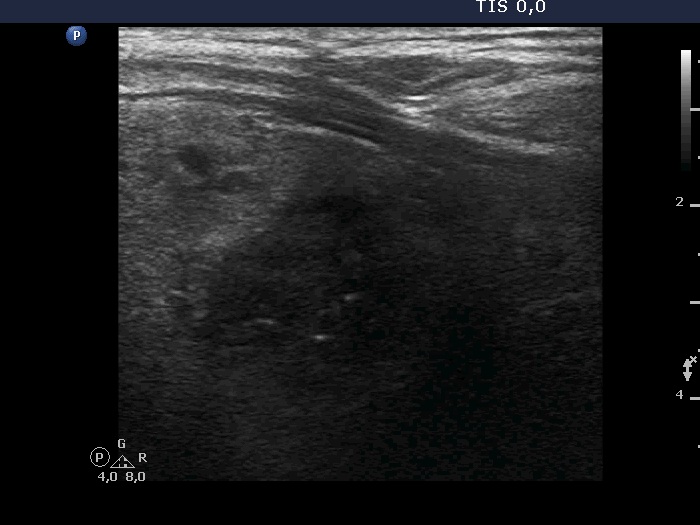
Four images gained on longitudinal scan are presented. The issue is the same as in the previous case: is it a discrete area composed of a single or multiple nodules. In my opinion, it is rather a single nodule: we can see on the left lower image an irregularly shaped echonormal area, the tail of which can be found even in the hypoechogenic part of the lesion.
|
| |
|
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
The issue is again the presence of multiple nodules: the entire nodular area seems to have lobulated margins, but in fact this is not a solitary nodule having lobulated margins but a cluster of smaller discrete lesions. |
| |
|
|
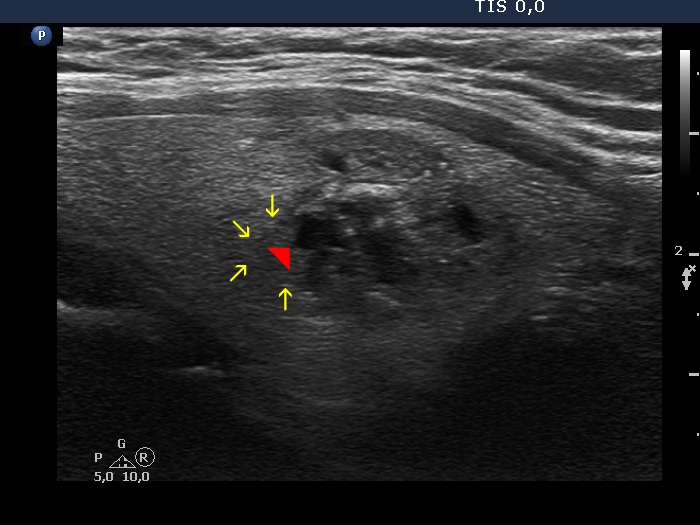 |
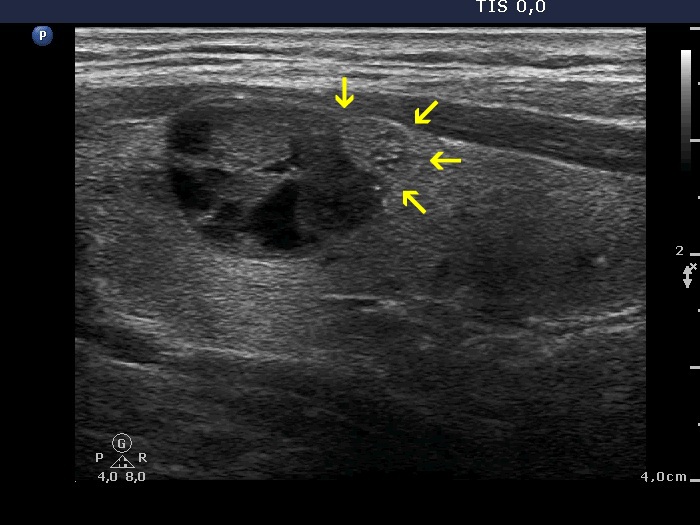
The red arrowhead points to a spiculation. We have to be aware of that this is found not in the border of a lesion but within a small nodule. The borders of this nodule are pointed with yellow arrows. Compared with the image, the video is more obvious regarding the real situation.
|
| |
|
|
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
There is no doubt about the irregular borders of the hypoechogenic discrete lesion. The issue is that this is only an internal part of large heterogeneous nodule which occupies almost the entire lobe. If we stand upon the definition of irregular borders than we should not group a nodule containing a discrete intranodular part with irregular surface among nodules presenting irregular borders.
|
| |
|
|
Transverse scan |
Longitudinal scan |
 |
 |
Two considerations. First, small irregularities of the borders should not be overestimated and the extent of irregularities has to be related to the size of the nodule. Second, large nodule occupying significant part of a lobe has no other chance than to follow the anatomical situation. The dorsomedial protrusion of the nodule is caused by the anatomy: the shape of the nodule simply fits to the shape of the lobe.
|
| |
|
Follicular adenoma in patient with Graves' disease (histology) - case 408 |
Transverse scans
|
 |
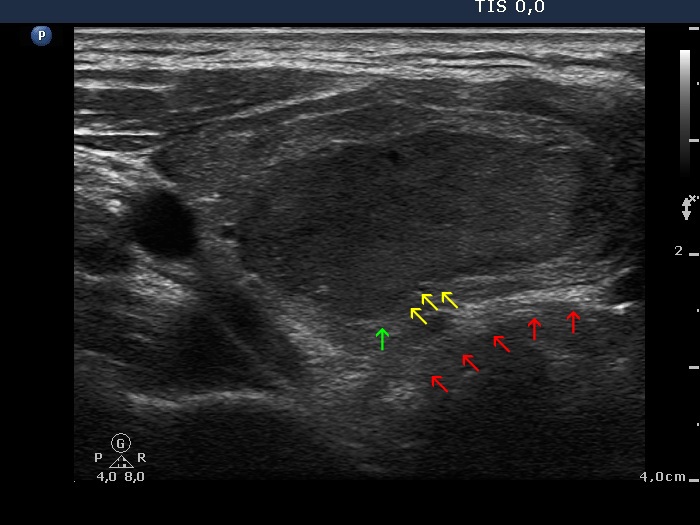 |
There are small irregularities all along on the nodule' borders. The degree of protrusions does not reach the level of pathological lobulation except for one marked with green. However, note that this protrusion is simply the consequence of the indentation (marked with yellow arrows) of the dorsal surface of the lobe. While the latter simply follows the arch of the trachea marked with red arrows.
|
|
First examination |
After the first session of sclerotherapy |
At the 4-year follow up |
 |
 |
 |
|
| Note that the projection (yellow arrows) of the cyst toward the isthmic part of the thyroid can be recognized even at the 4-year follow up when the nodule became significantly smaller. This projection simply followed the anatomical situation before the treatment and this distortion remained permanent. This projection should not be judged as a sign of abnormal, pathological border. We must be aware of the possibility of such pattern in nodules has been treated either with ethanol or laser of radiofrequency or in cyst which has been diminished with simple aspiration: the original distorted shape remains unchanged. |
| |
Benign, colloid goiter (cytology) - case 2152 |
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
Two forms of misleading patterns are demonstrated. First, the left ventral border of the nodule is spiculated (red arrow). But this is caused simply by the underlying anatomical situation, the narrowing end of the thyroid and should not be judged as irregular margin. The second issue is the protrusion in the medial part of the nodule which makes the appearance lobular. At first sight we could make a wrong judgement, however a bit more thorough analysis reveals that the protrusions are secondary, caused by an isoechoic small nodule (yellow arrows) which makes an impression on the surface of the larger, hypoechoic nodule.
|
| |
|
Benign, colloid goiter (cytology) - case 186 |
Transverse scan |
Longitudinal scan |
 |
 |
 |
 |
The medial (transverse scan) and the lower part (longitudinal scan) of the hypoechogenic nodule seems to lobulated or even spiculated. However, the cause of this irregularity is the impression of the border caused by echonormal lesion marked with yellow arrows.
|
| |
|
Recurrent hyperthyroidism after an insufficient surgery (clinical diagnosis) - case 17 |
Transverse scans (upper the right, lower the left lobe) |
Longitudinal scans (upper the right, lower the left lobe) |
 |
 |
 |
 |
A previous surgery has a deep impact on the anatomy of the thyroid: scars distort the normal shape of the gland, causing protrusions and spiculations. There is another issue in such cases: a central hypoechogenic part surrounded with thin echonormal tissue is one of the most frequent presentation of a subtotally resected thyroid. This pattern mimics as a large nodule would occupy almost the entire lobe. Be aware that all these circumstances, the hypoechoic pattern, the lobulated and spiculated surface of an apparent nodule might lead to overestimation the presentation as a highly suspicious one which is essentially an absolute normal finding. (This patient was reoperated, and histology disclosed no nodule.)
|
| |
|
|
Before the aspiration |
After the aspiration |
 |
 |
 |
 |
The shape and borders of the nodule were regular before the aspiration but became lobulated after the removal of the cystic fluid.
|
| |
|
|
Before the aspiration |
After the aspiration of 14 mL cystic fluid |
 |
 |
 |
 |
The situation is the same as in the previous case: the originally regular shape of the nodule became irregular after the removal of the cystic content: both spiculated and lobular forms have appeared bulging the nodule into the normal parenchyma.
|
|
|
