
PAPILLON COURSE on THYROID ULTRASOUNDSection 2 The nodular goiterPart 4 Intranodular echogenic figures
|
OPENING |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
I give an overview about the intranodular hyperechogenic figures. I discuss the various types, the differential diagnostics and their role in the evaluation and interpretation of various ultrasound patterns of thyroid nodules. These figures influence the judgment of thyroid nodules and are parts of the various TIRADS systems (1-4), they are involved in the indication of aspiration cytology and even the newest protocol emphasizes the role of correct interpretation of intranodular granules (5). The correct interpretation of these figures requires great experience but a paper textbook has its own limitation in an education process as we are required to analyze hundreds of videos and images to overview. In contrast with a handbook, a website has the capacity to present enough material for this purpose. I try to give a review of the literature and try to make one of the most important concerns clear about the published data: most authors behave as if not all of these hyperechogenic figures could be clearly categorized - which behavior in my opinion - is very far from the reality and might cause a feeling of insufficiency for less experienced readers. It is a very important dilemma: if we try to meet the requirement grouping each and every hyperechogenic figure, the professional background of our medical report will be affected. If we handle the issue appropriately, then the usefulness of TIRADS system might be questioned. In fact, in a significant proportion of cases an indisputable distinction is not possible. I only mention here one important fact. |
In contrast with other hyperechogenic figures, the probably most important one, the microcalcification has no specific feature: the diagnosis of a microcalcification is a matter of exclusion of other hyperechogenic figures which in contrast with microcalcification have their special properties. Yes, theoretically they share these signs, but in the everyday practice we often meet non-typical forms. So, in fact we only rarely can state with a nearly 100% probability that a figure is a microcalcification but our diagnosis has in almost all cases a given probability level. In this overview I try to profoundly discuss the ultrasound presentation and differentiation of connective tissue which ultrasound appearance is surprisingly underrepresented in publications. This is a stunner because connective tissue is the most frequent cause for a hyperechogenic granule and the differentiation between a microcalcification and a granule representing connective tissue is one of the most important differential diagnostic concerns in my experience. Also, in this selected topic I use the term punctate echogenic focus instead of microcalcification. I follow the tradition which uses the phrase microcalcification for one subgroup of hyperechogenic granules in other parts of the website and in case studies, but I am sure that it would be favorable if we replaced this term both because of scientific and ethical reasons. Regarding the first, more than 50% of microcalcifications described in an ultrasound report are in fact not microcalcifications in pathological terms. Regarding the ethical concerns, by the frequent misuse of the term microcalcification, we can cause great harm if a patient does research on the internet searching for "microcalcification". |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
THE IMPORTANCE AND THE SPECTRUM OF INTRANODULAR HYPERECHOGENIC FIGURES |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The presence of intranodular figures within a thyroid nodule might have a deep influence on the risk of malignancy. A microcalcification or an amyloid deposit significantly increases while the comet-tail artifact significantly decreases the risk of carcinoma. Moreover, the current algorithm of ETA emphasizes the issue of misclassification of these figures which might have an important impact even on the indication of FNAC (6). |
It means that the recognition and as exact as possible differentiation of intranodular hyperechogenic figures have great relevance in the everyday practice. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
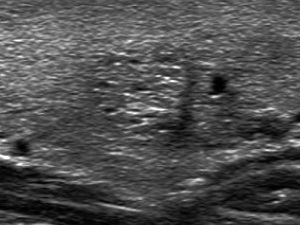
Connective tissue Connective tissue is the essential part of the human organs therefore we can find it in every thyroid nodule, as well. The ultrasound hallmark of connective tissue is the synchronous presence of lines and granules depending on the angle between the transducer and the connective tissue. A fine spiderweb-like pattern is almost always seen within nodules and is caused by thin and short pale lines and tiny granules (<1mm). We use the term non-specific hyperechogenic figure for this normal finding. |
Also, it is more difficult to visualize or if it is visualized, then to appreciate a linear or curved structure than a granule because the former requires that we place the transducer almost parallel of the structure, so in most cases of fibrosis the granules predominate over lines. It means that an important differential diagnostic problem arises in the predominance of hyperechogenic granules: the differentiation between microcalcification and proliferation of the connective tissue. Except for the localization, the presentation of this echogenic figure is identical with that of back wall cystic figures. However, proliferation of connective tissue is found in solid parenchyma while the latter in the dorsal wall of cystic areas. The distinction between these figures is not always possible, but it has minimal if any relevance. There is only very limited mentioning of this figure in the literature, therefore, in contrast with most figures, there is only limited data available about the likelihood of this malignancy. Beland et al. have found no malignancies among 29 nodules presenting linear echogenic foci (6), which is in accordance with our finding: the intranodular presence of connective tissue neither decreases nor increases the likelihood of the malignancy. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Comet-tail artifacts or colloid crystals The so-called comet-tail artifact is very similar to the microcalcification, it is similarly bright, the size is in the range of microcalcification, although tends to be larger and occasionally exceeds 1 cm. The shape of a colloid crystal is in most cases round, however line |
The issue is the appearance of non-typical forms within a solid nodule or within the solid part of a mixed nodule. Comet-tail artifacts are generally held as a sign which suggest that the lesion is benign with great probability (6-8). (7: 0/45, 6: 0/19, 8: 0/31). There is a group of investigators who have described an extremely great malignancy rate among nodules presenting comet-tail artifact: Malhi et al. have found a 15.4% (34/221) and a 3.9% (2/52) carcinoma rate, nodules with small (=1mm long) and large (>1mm long) comet-tail artifacts, respectively (9). The malignancy rate was even higher in hypoechogenic nodules: 27.6% (27/98) and 20% (2/10), nodules with small (=1mm long) and large (>1mm long) comet-tail artifacts, respectively. This publication cannot be ignored because the authors presented good quality images of 3 malignant cases undoubtedly having comet-tail artifacts.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Posterior back wall enhancement |
caused by colloid crystals or posterior acoustic enhancement of the back wall of a microcystic area. These may be confused with microcalcifications by less proficient sonographers, and a recent meta-analysis confirmed that operator experience is correlated with accurate evaluation of internal calcifications (10). Therefore, because of potential for misclassification, FNA may still be considered interpreted as spongiform for nodules, but with a higher size cutoff (5). So the importance of this optical illusion lies in the potential misinterpretation by less trained researchers as microcalcification. The tiny cystic areas are not infrequently very difficult to find, which might lead to a differential diagnostic issue if granules predominate the pattern. In contrast with all other hyperechogenic figures this is not a real structure but only an optical artifact. (In the event of comet-tail artifact, the colloid crystal is a real figure only the tail is the artifact.) |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Punctate echogenic foci (including microcalcifications) This group includes the most important hyperechogenic figure, the microcalcification. Small (=1mm) bright, |
true microcalcification is occasionally seen not as a round but a bit elongated structure depending on the equipment and the settings used, the depth of the figure, the surrounding parenchyma which all influence the optical appearance of a microcalcification. The term "microcalcification" is often misleading but it has been traditionally used for decades for punctate echogenic foci. The ultrasound and pathological denomination of microcalcification is not the same. In pathology microcalcifications are found almost exclusively in papillary carcinoma, but in ultrasound microcalcification is used for every hyperechogenic granules. This is occasionally a typical "post hoc ergo propter hoc" situation: we present in textbooks/publications/websites ultrasound images of histologically verified papillary carcinomas and state that these granules are microcalcifications. However, prospective studies prove that the absolute number of benign lesions containing punctate echogenic foci is higher than that of malignant cases. The details of 10 publications show that the medians of nodules contained microcalcifications were 4.1% and 45.5%, histologically verified benign and malignant nodules, respectively (7,11-19). See Table 2. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Considering that in contrast with malignant nodules, great proportions of benign nodules are treated conservatively, the absolute number of "microcalcifications" in benign nodules is much higher. Theoretically a microcalcification corresponds to calcification of a tip of a papillary fragment. The cause for calcification is degeneration and/or a worsening vascular supply of the cells located at the edge of a papillary cluster. On the other hand, there is no direct proof that a bright hyperechogenic spot seen on ultrasound indeed corresponds to microcalcification. Moreover, similar ultrasound granules can be found in high proportion of hyperplastic nodules without any calcifications which suggests that any papillary fragment might present as "microcalcification" on ultrasound; a punctate echogenic focus might represent condensation of nuclei. (If we analyze a papillary fragment the nuclei are more densely located at the periphery than in the center of the cell group.) An earlier study (20) explored the origins of similar punctate echogenic foci in the ovary and concluded that they are often the result of specular reflections from the back walls of tiny unresolved cysts and not psammomatous calcifications at all. I absolutely agree with Malhi et al. who "believe that calling these punctate echogenic foci microcalcifications is a misnomer" (9). The inappropriate use of phrase microcalcification is not only scientifically unfounded but might lead to unnecessary anxiety and even to unnecessary and otherwise unfounded |
operations. The current guideline of the ETA (2) on nodular goiter uses the category of "True microcalcifications" but fails to describe in detail how to differentiate this category from "Hyperechogenic spots of uncertain significance". This is not a surprise because there is no publication in the literature which would verify a clear distinction between these two categories. (I try to use consistently the term "punctate echogenic foci" in the text and courses of this selected topic, however in case studies I use the term microcalcification for bright granules between 0.5 and 1 mm in size and without a tail or without the synchronous presence of hyperechogenic lines.) In my opinion, the terminology of the American College of Radiology is more appropriate, they use the phrase "punctate echogenic foci" instead of microcalcification (4). |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Coarse calcification
|
We have to mention the eggshell-calcification or peripheral rim calcification. This corresponds to calcification of the ca |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Amyloid deposit |
There is no general agreement about the origin of this figure. Many authors neglect its typical presentation of this special figure and group them simply among coarse calcifications. E.g., very typical ultrasound images of medullary carcinoma presenting this typical pattern were published in three recent articles and the authors simply notice that the lesion has calcification (Fig.2A in ref. 30, Fig.1 in ref. 31 and Fig.16b in ref 32). I highly advise to review Fig.2A in Trimboli's article (30): the nodule has a large hyperechogenic patch in the central part which lacks dorsal acoustic shadow: it is hard to imagine such a great focus of calcification without acoustic shadowing. The situation is similar in the article of Hoang et al. (32): a typical patch is demonstrated in Fig.16b which lacks dorsal acoustic shadowing. In my opinion and practice the identification of such compound patches without an acoustic shadow has a high specificity and sensitivity for medullary carcinoma, but if these patches have an acoustic shadow, these parameters are worse though high enough to raise the suspicion of medullary cancer. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Granulation around surgical thread Granulation around surgical thread might appear even decades after a previous surgery. This is a hypoechogenic lesion containing hyperechogenic figures of various sizes usually within a less hypoechogenic ragged tissue fragment. The lesion is always avascular and the shape is always irregular. We frequently find acoustic shadow dorsal to a granulation which might be caused by the thick scar. The presence of occasionally small, bright hyperechogenic granules within a hypoechogenic, hard lesion might be misleading first of all if the patient was previously operated on papillary carcinoma or if the radiologist is not |
aware of a pre  vious surgery. The other differential diagnostic problem might arise in a patient previously operated on medullary carcinoma; the recurrence of the tumor might have identical ultrasound presentation as a benign granulation. vious surgery. The other differential diagnostic problem might arise in a patient previously operated on medullary carcinoma; the recurrence of the tumor might have identical ultrasound presentation as a benign granulation.This figure is only rarely mentioned in the literature (33) and various terms are used describing this entity as suture granuloma (34) or foreign-body granuloma (35). |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
MICROCALCIFICATIONS IN THE MOST FREQUENT SUBTYPES OF THYROID CARCINOMAS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Microcalcifications are known as characteristic feature of papillary cancer. However, the occurrence of them is similarly high in medullary carcinoma. These data in Table 3 show the incidence on ultrasound. Of course, it can |
be debated that the dots identified as microcalcification in medullary cancer are indeed microcalcifications. As with most suspicious ultrasound features, microcalcification is much less common in follicular carcinoma. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
THE ROLE OF INTRANODULAR ECHOGENIC FIGURES IN VARIOUS TIRADS |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
The presence of microcalcification automatically groups the lesion among the most suspicious subgroup in the AACE and in the European TIRADS, while a lesion presenting microcalcifications has to put either to the most but one or most suspicious category in the ATA and Korean TIRADS, isoechoic or hypoechoic nodules, respectively. Regarding the ACR TIRADS, the term 'punctate echogenic foci' is used for microcalcifications and short-tail comet-tail artifacts and worth three points. Following the logic of this system, it means that almost all lesions presenting this feature should be categorized into category 5. (See Table 4.) The presence of macrocalcification has no role in three TIRADS. While it is worth one or three points in ACR TIRADS, macrocalcification or peripheral (rim) calcification, respectively. It means that ACR treats rim calcification in a similar way to widely accepted suspicious sign; an approach which is not backed by scientific data. Rim calcifications with extrusive soft tissue component is enlisted among the most suspicious characteristics in the ATA TIRADS. |
It is interesting that comet-tail artifacts are handled differently in various TIRADS. At the one end is the Korean TIRADS which groups all nodules presenting comet-tail artifact among the possible lowest category, if comet-tail artifact is found in cystic portion and the nodule lacks suspicious US characteristics. Although AACE mentions comet tail artifacts among features characteristic for benign lesions, the lack or presence of comet tail artifact does not influence the classification of nodules in AACE. In the event of ACR TIRADS large comet-tail artifacts worth 0 points, while short comet-tail artifacts in the solid part worth the maximal as possible 3 points because this is included in the punctate echogenic foci feature. Considering the difficulties of the correct judgement of comet-tail artifacts, neither the Korean nor the ACR approach seems to be moderate enough, the former might lead to underestimation of a nodule presenting comet-tail artifacts while the latter might lead to overestimation. Until we reach a significantly better agreement in the judgement of this characteristic, the more restrained handling of this sign by the ATA, ETA (they do not involve comet tail artifacts in their system) and AACE seems more well-founded". |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
THE DIFFERENTIATION OF THE VARIOUS INTRANODULAR HYPERECHOGENIC GRANULES |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
In this chapter we focus on the differentiation of hyperechogenic granules because other figures have their own hallmarks, the dorsal acoustic shadow, the synchronous presence of hyperechogenic lines and granules and the characteristic clinical and ultrasound pattern described above, coarse calcification, fibrosis and granulation around surgical thread, respectively. In the everyday practice the issue is very simple to frame: we need to decide if an actual hyperechogenic granule is a punctate echogenic focus (microcalcification) or not. Moreover, this issue might arise only in the event of figures located in a solid nodule or in the solid part of a mixed lesion (27). We have to understand that the identification of a punctate echogenic focus is a matter of exclusion because in contrast with all other hyperechogenic figures a microcalcification has no pathognomonic presentation: a hyperechogenic granule might be a non-typical form of a colloid crystal or a granular presentation of connective tissue. It is evident that a hyperechogenic granule within a cystic area has no oncological relevance. There are several general rules. Firstly, if a lesion presents numerous and various hyperechogenic granules we have to analyze all of them and not a single one. Secondly, in certain cases the analysis of other nodules might be of help in differential diagnostic of hyperechogenic figures. Finally, there is not one ultrasound feature which itself can prove or exclude thyroid carcinoma. We have to interpret the single features with others. In this context, the presence of microcalcification is one of the most important finding in thyroid ultrasound which increases the likelihood of malignancy. Regarding the first rule, if a lesion contains several typical comet-tail artifacts, then bright granules without a tail belong very likely also to this subgroup. |
Granules with similar brightness and size very likely correspond to the same subtype. Another example: microcalcifications almost always coexist with tiny pale granules. In the event of a granulation around surgical thread, we frequently found bright granules but these occur within a larger patch-like echonormal structures. Tiny punctate echogenic foci (microcalcifications) cannot be differentiated from non-specific granulations of connective tissue except for those cases when synchronous short hyperechogenic lines are also present which stands for a non-specific granule. In doubtful cases the finding of similar but unequivocal hyperechogenic figure in a different nodule having an identical echogenicity might be of great help. As regards the second rule, if we found multiple nodules with the same echo pattern, then the hyperechogenic figures of similar size and brightness very likely belong to the same subtype. So, an ambiguous granule in one lesion is also very likely a comet-tail artifact if we found typical comet-tail artifact in another nodule. Regarding the third consideration, in order to find a single punctate echogenic focus within an echonormal nodule showing regular shape and borders is an absolutely different story compared with a hypoechogenic nodule presenting a starry sky phenomenon and having blurred, irregular borders and a lobulated surface. I emphasize that we are not able to differentiate each and every hyperechogenic granule and the interobserver variation must be very high. |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 Thick and bright hyperechogenic granules and lines are signs of thickened connective tissue.
Thick and bright hyperechogenic granules and lines are signs of thickened connective tissue. 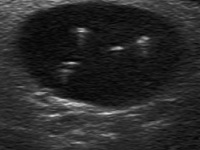 ar form is not a rare exception. The most important feature differentiating a comet-tail artifact from a microcalcification is the presence of a narrowing and fading tail in the former. Although colloid crystals typically appear in the cystic part of a mixed solid-cystic lesion, we must be aware that comet-tail artifact might be located even within the solid part and the differentiation of bright granules in a solid lesion is the other important differential diagnostic issue regarding hyperechogenic figures. Comet-tail artifact is generally held a protein-rich structure or a colloid crystal.
ar form is not a rare exception. The most important feature differentiating a comet-tail artifact from a microcalcification is the presence of a narrowing and fading tail in the former. Although colloid crystals typically appear in the cystic part of a mixed solid-cystic lesion, we must be aware that comet-tail artifact might be located even within the solid part and the differentiation of bright granules in a solid lesion is the other important differential diagnostic issue regarding hyperechogenic figures. Comet-tail artifact is generally held a protein-rich structure or a colloid crystal.  This figure is an optical artifact and is seen exclusively in the dorsal wall and occasionally in the parenchyma just dorsal to a cystic area. The cause of this figure is the enhancement of ultrasound reflection. Spongiform and other mixed cystic solid nodules may exhibit bright reflectors on US imaging,
This figure is an optical artifact and is seen exclusively in the dorsal wall and occasionally in the parenchyma just dorsal to a cystic area. The cause of this figure is the enhancement of ultrasound reflection. Spongiform and other mixed cystic solid nodules may exhibit bright reflectors on US imaging,  round granules without a dorsal tail and without the concomitant presence of similarly bright lines belong to this subgroup. It is crucial to be aware about the fact that in contrast with other hyperechogenic figures, punctate echogenic foci (microcalcifications) lack a specific pattern. A hyperechogenic bright spot can be seen in all other forms of hyperechogenic figures but these have additional features, as well. Unfortunately, they only use to have these additional features, and here it comes the differential diagnostic issue: if we see only hyperechogenic granules, theoretically we cannot exclude the possibility of non-typical presentation of a colloid crystal or connective tissue. And there is another problem, on ultrasound a
round granules without a dorsal tail and without the concomitant presence of similarly bright lines belong to this subgroup. It is crucial to be aware about the fact that in contrast with other hyperechogenic figures, punctate echogenic foci (microcalcifications) lack a specific pattern. A hyperechogenic bright spot can be seen in all other forms of hyperechogenic figures but these have additional features, as well. Unfortunately, they only use to have these additional features, and here it comes the differential diagnostic issue: if we see only hyperechogenic granules, theoretically we cannot exclude the possibility of non-typical presentation of a colloid crystal or connective tissue. And there is another problem, on ultrasound a 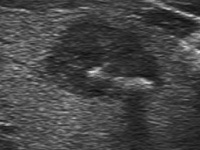 The next typical hyperechogenic figure is the coarse calcification. The shape is linear or curved or might be granular. In smaller foci it might seem to be round. It ranges from 1 mm to several cm and presents a dorsal acoustic shadow. The latter is the ultrasound hallmark of coarse calcification. Often, we did not find the calcified focus and only the dorsal acoustic shadow proves the existence of calcification. According to recent studies, macrocalcifications within a nodule, if combined with microcalcifications, confer the same malignancy risk as microcalcifications alone (18,21) refers the current guideline of the ATA (5), while just the opposite states the newest guideline of ETA: "microcalcifications are highly suggestive of malignancy, in particular when associated with macrocalcifications" (1). The presence of intranodular (central) macrocalcification alone is not consistently associated with thyroid cancer (23). Calcification represents perhaps a possible pathologic evolution of some thyroid lesions (24).
The next typical hyperechogenic figure is the coarse calcification. The shape is linear or curved or might be granular. In smaller foci it might seem to be round. It ranges from 1 mm to several cm and presents a dorsal acoustic shadow. The latter is the ultrasound hallmark of coarse calcification. Often, we did not find the calcified focus and only the dorsal acoustic shadow proves the existence of calcification. According to recent studies, macrocalcifications within a nodule, if combined with microcalcifications, confer the same malignancy risk as microcalcifications alone (18,21) refers the current guideline of the ATA (5), while just the opposite states the newest guideline of ETA: "microcalcifications are highly suggestive of malignancy, in particular when associated with macrocalcifications" (1). The presence of intranodular (central) macrocalcification alone is not consistently associated with thyroid cancer (23). Calcification represents perhaps a possible pathologic evolution of some thyroid lesions (24).  psule of a lesion. There are conflicting studies whether this feature would increase the risk of malignancy. Certainly, if it does, then more in a statistical than in a practical sense. However, a nodule that has interrupted peripheral calcifications, in association with a soft tissue rim outside the calcification, has been reported highly likely to be malignant, and the associated pathology may demonstrate tumor invasion in the area of disrupted calcification (25-27). The issue is that a direct tumor spread is only rarely unequivocal on ultrasound. In the TIRADS of the American College of Radiology macrocalcifications is worth 1 point, while peripheral (rim) calcification is worth 2 points (see
psule of a lesion. There are conflicting studies whether this feature would increase the risk of malignancy. Certainly, if it does, then more in a statistical than in a practical sense. However, a nodule that has interrupted peripheral calcifications, in association with a soft tissue rim outside the calcification, has been reported highly likely to be malignant, and the associated pathology may demonstrate tumor invasion in the area of disrupted calcification (25-27). The issue is that a direct tumor spread is only rarely unequivocal on ultrasound. In the TIRADS of the American College of Radiology macrocalcifications is worth 1 point, while peripheral (rim) calcification is worth 2 points (see  An amyloid deposit has a specific cotton-like patchy appearance (28, 29). We have found this compound figure 118 times more frequently in medullary carcinoma compared with other thyroid malignancies: 48% 11/23 (48%) and 4/463 (0.9%), medullary carcinoma and other thyroid carcinomas, respectively (29). These patches have a composite structure, might contain punctate echogenic foci and occasionally present dorsal acoustic shadow. The cause for the latter might be coarse calcification but a thick amyloid might also hinder the penetration of an ultrasound wave. Similar structures occur even in degenerative hyperplastic nodules when small echonormal areas appear within a hypoechogenic lesion. However, most of the latter, benign cases lack granulations. However, a granulation around a surgical thread might have an identical pattern to amyloid.
An amyloid deposit has a specific cotton-like patchy appearance (28, 29). We have found this compound figure 118 times more frequently in medullary carcinoma compared with other thyroid malignancies: 48% 11/23 (48%) and 4/463 (0.9%), medullary carcinoma and other thyroid carcinomas, respectively (29). These patches have a composite structure, might contain punctate echogenic foci and occasionally present dorsal acoustic shadow. The cause for the latter might be coarse calcification but a thick amyloid might also hinder the penetration of an ultrasound wave. Similar structures occur even in degenerative hyperplastic nodules when small echonormal areas appear within a hypoechogenic lesion. However, most of the latter, benign cases lack granulations. However, a granulation around a surgical thread might have an identical pattern to amyloid.References
1. Russ G, Bonnema SJ, Erdogan MF, Durante C, Ngu R, Leenhardt L. European Thyroid Association Guidelines for Ultrasound Malignancy Risk Stratification of Thyroid Nodules in Adults: The EU-TIRADS. Eur Thyroid J. 2017 Sep;6(5):225-237. doi: 10.1159/000478927.
2. Russ G, Leboulleux S, Leenhardt L, Hegedüs L. Thyroid Incidentalomas: Epidemiology, Risk Stratification with Ultrasound and Workup. Eur Thyroid J. 2014 Sep; 3(3): 154-163. doi: 10.1159/000365289
3. Gharib H, Papini E, Garber JR, Duick DS, Harrell RM, Hegedüs L, Paschke R, Valcavi R, Vitti P. AACE/ACE/AME Task Force on Thyroid Nodules: American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules - 2016 update. Endocr Pract 2016; 22:622-639. doi: 10.4158/EP161208.GL
4. Tessler FN, Middleton WD, Grant EG, Hoang JK, Berland LL, Teefey SA, Cronan JJ, Beland MD, Desser TS, Frates MC, Hammers LW, Hamper UM, Langer JE, Reading CC, Scoutt LM, Stavros AT. ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the ACR TI-RADS Committee. J Am Coll Radiol. 2017 May;14(5):587-595. doi: 10.1016/j.jacr.2017.01.046. Full text in pdf
5. Haugen BR, Sawka AM, Alexander EK, Bible KC, Caturegli P, Doherty GM, Mandel SJ, Morris JC, Nassar A, Pacini F, Schlumberger M0, Schuff K, Sherman SI, Somerset H, Sosa JA, Steward DL, Wartofsky L, Williams MD. American Thyroid Association Guidelines on the Management of Thyroid Nodules and Differentiated Thyroid Cancer Task Force Review and Recommendation on the Proposed Renaming of Encapsulated Follicular Variant Papillary Thyroid Carcinoma Without Invasion to Noninvasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features. Thyroid. 2017 Apr;27(4):481-483. doi: 10.1089/thy.2016.0628.
6. Beland MD, Kwon L, Delellis RA, Cronan JJ, Grant EG. Nonshadowing echogenic foci in thyroid nodules: are certain appearances enough to avoid thyroid biopsy? J Ultrasound Med. 2011 Jun;30(6):753-60. doi: 10.7863/jum.2011.30.6.753.
7. Zayadeen AR, Abu-Yousef M, Berbaum K. JOURNAL CLUB: Retrospective Evaluation of Ultrasound Features of Thyroid Nodules to Assess Malignancy Risk: A Step Toward TIRADS. AJR Am J Roentgenol. 2016 Sep;207(3):460-9. doi: 10.2214/AJR.15.15121.
8. Kim DW, Park JS, In HS, Choo HJ, Ryu JH, Jung SJ. Ultrasound-based diagnostic classification for solid and partially cystic thyroid nodules. AJNR Am J Neuroradiol. 2012 Jun;33(6):1144-9. doi: 10.3174/ajnr.A2923.
9. Malhi H, Beland MD, Cen SY, Allgood E, Daley K, Martin SE, Cronan JJ, Grant EG. Echogenic Foci in Thyroid Nodules: Significance of Posterior Acoustic Artifacts. AJR Am J Roentgenol. 2014 Dec;203(6):1310-6. doi: 10.2214/AJR.13.11934.
10. Brito JP, Gionfriddo MR, Al Nofal A, Boehmer KR, Leppin AL, Reading C, Callstrom M, Elraiyah TA, Prokop LJ, Stan MN, Murad MH, Morris JC, Montori VM. The Accuracy of Thyroid Nodule Ultrasound to Predict Thyroid Cancer: Systematic Review and Meta-Analysis. J Clin EndocrinolMetab 2014 Apr;99(4):1253-63. doi: 10.1210/jc.2013-2928.
11. Kim EK, Park CS, Chung WY, Oh KK, Kim DI, Lee JT, Yoo HS. New sonographic criteria for recommending fine-needle aspiration biopsy of nonpalpable solid nodules of the thyroid. AJR Am J Roentgenol. 2002 Mar;178(3):687-91. doi: 10.2214/ajr.178.3.1780687.
12. Cappelli C, Castellano M, Pirola I, Gandossi E, De Martino E, Cumetti D, Agosti B, Rosei EA. Thyroid nodule shape suggests malignancy. Eur J Endocrinol. 2006 Jul;155(1):27-31. doi: 10.1530/eje.1.02177.
13. Gulcelik NE, Gulcelik MA, Kuru B. Risk of malignancy in patients with follicular neoplasm: predictive value of clinical and ultrasonographic features. Arch Otolaryngol Head Neck Surg. 2008 Dec;134(12):1312-5. doi: 10.1001/archotol.134.12.1312.
14. Salmaslioglu A, Erbil Y, Dural C, Iºsever H, Kapran Y, Ozarma?an S, Tezelman S. Predictive value of sonographic features in preoperative evaluation of malignant thyroid nodules in a multinodular goiter. World J Surg. 2008 Sep;32(9):1948-54. doi: 10.1007/s00268-008-9600-2.
15. Popowicz B, Klencki M, Lewiñski A, Slowiñska-Klencka D. The usefulness of sonographic features in selection of thyroid nodules for biopsy in relation to the nodule's size. Eur J Endocrinol. 2009 Jul;161(1):103-11. doi: 10.1530/EJE-09-0022.
16. Sharma A, Gabriel H, Nemcek AA, Nayar R, Du H, Nikolaidis P. Subcentimeter thyroid nodules: utility of sonographic characterization and ultrasound-guided needle biopsy. AJR Am J Roentgenol. 2011 Dec;197(6):W1123-8. doi: 10.2214/AJR.10.5684.
17. Ozel A, Erturk SM, Ercan A, Ylmaz B, Basak T, Cantisani V, Basak M, Karpat Z. The diagnostic efficiency of ultrasound in characterization for thyroid nodules: how many criteria are required to predict malignancy? Med Ultrason. 2012 Mar;14(1):24-8. doi: http://www.medultrason.ro/assets/Medultrason-2012-vol14-no1/05Ozel.pdf
18. Papini E, Guglielmi R, Bianchini A, Crescenzi A, Taccogna S, Nardi F, Panunzi C, Rinaldi R, Toscano V, Pacella CM. Risk of malignancy in nonpalpable thyroid nodules: predictive value of ultrasound and color-Doppler features. J Clin Endocrinol Metab. 2002 May;87(5):1941-6. doi: 10.1210/jcem.87.5.8504.
19. Solymosi T, Lukacs-Toth L, Nagy D, Gal I. A Prospective Study on 3,907 Patients with Thyroid Nodules. Sono-histological Comparison and the Controversial Significance of the Halo Sign in Predicting Thyroid Malignancy. Br J Med Med Res. 2015; 5.8: 1053-1059. doi: 10.9734/BJMMR/2015/13743.
20. Muradali D, Colgan T, Hayeems E, Burns PN, Wilson SR. Echogenic ovarian foci without shadowing: are they caused by psammomatous calcifications? Radiology. 2002 Aug;224(2):429-35. doi: 10.1148/radiol.2242911110.
21. Moon WJ, Jung SL, Lee JH, Na DG, Baek JH, Lee YH, Kim J, Kim HS, Byun JS, Lee DH; Thyroid Study Group, Korean Society of Neuro- and Head and Neck Radiology. Benign and malignant thyroid nodules: US differentiation--multicenter retrospective study. Radiology. 2008 Jun;247(3):762-70. doi: 10.1148/radiol.2473070944.
22. Moon WJ, Baek JH, Jung SL, Kim DW, Kim EK, Kim JY, Kwak JY, Lee JH, Lee JH, Lee JH, Na DG, Park JS, Park SW. Ultrasonography and the Ultrasound-Based Management of Thyroid Nodules: Consensus Statement and Recommendations. Korean J Radiol. 2011 Jan-Feb; 12(1): 1-14. doi: 10.3348/kjr.2011.12.1.1.
23. Moon HJ, Sung JM, Kim EK, Yoon JH, Youk JH, Kwak JY. 2012. Diagnostic performance of gray-scale US and elastography in solid thyroid nodules. Radiology 262:1002-1013. doi: 10.1148/radiol.11110839.
24. Solbiati L, Osti V, Cova L, Tonolini M. Ultrasound of thyroid, parathyroid glands and neck lymph nodes. Eur Radiol. 2001;11(12):2411-24. doi: 10.1007/s00330-001-1163-7.
25. Kim DS, Kim JH, Na DG, Park SH, Kim E, Chang KH, Sohn CH, Choi YH. Sonographic features of follicular variant papillary thyroid carcinomas in comparison with conventional papillary thyroid carcinomas. J Ultrasound Med. 2009 Dec;28(12):1685-92. doi: 10.7863/jum.2009.28.12.1685.
26. Park YJ, Kim JA, Son EJ, Youk JH, Kim EK, Kwak JY, Park CS. Thyroid nodules with macrocalcification: sonographic findings predictive of malignancy. Yonsei Med J. 2014 Mar;55(2):339-44. doi: 10.3349/ymj.2014.55.2.339.
27. Andrioli M, Chiara Carzaniga C, Persani L. Standardized Ultrasound Report for Thyroid Nodules: The Endocrinologist's Viewpoint. Eur Thyroid J. 2013 Mar; 2(1): 37-48. doi: 10.1159/000347144.
28. Gorman B, Charboneau JW, James EM, Reading CC, Wold LE, Grant CS, Gharib H, Hay ID. Medullary thyroid carcinoma: role of high-resolution US. Radiology. 1987 Jan;162(1 Pt 1):147-50. doi: 10.1148/radiology.162.1.3538147.
29. Solymosi T, Lukacs Toth G, Nagy D, Gal I. Twenty years of experience with the preoperative diagnosis of medullary cancer in a moderately iodine-deficient region. Int J Endocrinol. 2013;2013:571606. doi: 10.1155/2013/571606.
30. Trimboli P, Giovanella L, Valabrega S, Andrioli M, Baldelli R, Cremonini N, Rossi F, Guidobaldi L, Barnabei A, Rota F, Paoloni A, Rizza L, Fattorini G, Latini M, Ventura C, Falasca P, Orlandi F, Crescenzi A, D'Ambrosio F, Cantisani V, Romanelli F, Negro R, Saggiorato E, Appetecchia M. Ultrasound features of medullary thyroid carcinoma correlate with cancer aggressiveness: a retrospective multicenter study. J Exp Clin Cancer Res. 2014 Oct 25;33:87. doi: 10.1186/s13046-014-0087-4.
31. Kim SH, Kim BS, Jung SL, Lee JW, Yang PS, Kang BJ, Lim HW, Kim JY, Whang IY, Kwon HS, Jung CK. Ultrasonographic findings of medullary thyroid carcinoma: a comparison with papillary thyroid carcinoma. Korean J Radiol. 2009 Mar-Apr;10(2):101-5. doi: 10.3348/kjr.2009.10.2.101.
32. Hoang JK, Lee WK, Lee M, Johnson D, Farrell S. US Features of thyroid malignancy: pearls and pitfalls. Radiographics. 2007 May-Jun;27(3):847-60; discussion 861-5. doi: 10.1148/rg.273065038.
33. Zaheer S, Tan A, Ang ES, Loke KS, Kao YH, Goh A, Wong WY. Post-thyroidectomy neck ultrasonography in patients with thyroid cancer and a review of the literature. Singapore Med J. 2014 Apr;55(4):177-183. doi: 10.11622/smedj.2014050.
34. Rettenbacher T, Macheiner P, Hollerweger A, Gritzmann N, Weismann C, Todoroff B. Suture granulomas: sonography enables a correct preoperative diagnosis. Ultrasound Med Biol. 2001 Mar;27(3):343-50. Ultrasound Med Biol. 2001 Mar;27(3):343-50. doi: 10.1016/S0301-5629(00)00364-1
35 Ko MS, Lee JH, Shong YK, Gong GY, Baek JH. Normal and abnormal sonographic findings at the thyroidectomy sites in postoperative patients with thyroid malignancy. AJR Am J Roentgenol. 2010 Jun;194(6):1596-609. doi: 10.2214/AJR.09.2513.