
PAPILLON COURSE on THYROID ULTRASOUNDSection 2 The nodular goiterPart 1 Introduction to chapter nodular goiter
|
OPENING |
|||||||||||||||||||||||||||||||||||||
This chapter discusses the diagnosis of thyroid nodule and multinodular goiter and the treatment of benign forms. |
Thyroid nodules are one of the most common endocrine disorders; they are mostly benign; however, the diagnosis of malignancy is a crucial issue. |
||||||||||||||||||||||||||||||||||||
DEFINITION OF THE DISEASE |
|||||||||||||||||||||||||||||||||||||
Thyroid nodule (TN) is one of the most common endocrine abnormalities: Palpable nodules are found in 4-7% of the normal population, while discrete lesions can be found in almost every adult. Less than 1% of the thyroid lesions can be life-threatening due to their malignant potential. The evaluation of TNs became quite simple as TSH determination, thyroid ultrasound (US), and fine needle aspiration cytology (FNA) are enough for a complete diagnosis in most cases. One of the main issues is that the US and the FNA are both highly dependent on the examiner, and in contrast to cardiology, US is usually performed not by a specialist of the field but by a radiologist. TNs cannot |
be treated with drugs; therefore, the basic question regarding a patient with thyroid nodule is whether to operate or not. Recently, nonsurgical methods are getting increasingly available. One of the main issues is that the US and the FNA are both highly dependent on the examiner, and in contrast to cardiology, US is usually performed not by a specialist of the field but by a radiologist. TNs cannot be treated with drugs; therefore, the basic question regarding a patient with thyroid nodule is whether to operate or not. Recently, nonsurgical methods are getting increasingly available. |
||||||||||||||||||||||||||||||||||||
HOW TO DEFINE A THYROID NODULE? |
|||||||||||||||||||||||||||||||||||||
As many methods of examination exist, the nodular goiter is defined in so many different ways. Traditionally, palpation was the basis of the diagnosis. Recently, a TN is determined by US. The issue is that every thyroid disorder, not only TN, appears in the form of discrete lesions, e.g., the most common US sign of autoimmune thyroiditis is the presence of discrete lesions which involve more than 90% of Hashimoto thyroiditis patients. If the nodule was defined as a discrete US lesion, most adult humans would be labeled as nodular goiter patients. |
In order to avoid psychological harm and unnecessary cost, we need to separate lesions that are histologically nodules from those that are not, or we have to determine which lesion needs further investigation and which one does not. Although there is no consensus among experts on how to do this, most protocols determine a maximum diameter of discrete lesions. We do not use the term nodule or do not perform further diagnostic tests below that size. The size limit is 10 mm for those lesions which do not present suspicious signs and 5 mm for those which do. |
||||||||||||||||||||||||||||||||||||
WHAT ARE THE CLINICAL SIGNS OF AN ENLARGED THYROID? |
|||||||||||||||||||||||||||||||||||||
A persistent problem with swallowing when consuming solid food is the most reliable and common sign for an enlarged thyroid gland. The cartilaginous-walled trachea is harder to compress with the goiter than the muscular-walled esophagus. Therefore, it is less likely that an enlarged thyroid would cause dyspnea without a swallowing problem. Tracheal X-ray examination is of great help in uncertain cases. Deeper voice is experienced in a thyroid gland of a significant size, as well. |
Palsy of the recurrent nerve confirmed by a laryngeal examination in any case raises the suspicion of thyroid cancer. In contrast to the former symptoms, the most frequent neck complaint, the 'lump in the throat feeling', is usually not caused by a thyroid disease. This is caused by an increase blood supply in the thyroid due to physical or mental issues, which is experienced by a 10-15% of the population. |
||||||||||||||||||||||||||||||||||||
WHAT ARE THE GOALS OF EVALUATION IN THYOID NODULES? HOW TO EVALUATE A PATIENT WITH A SUSPERCETED NODULE? |
|||||||||||||||||||||||||||||||||||||
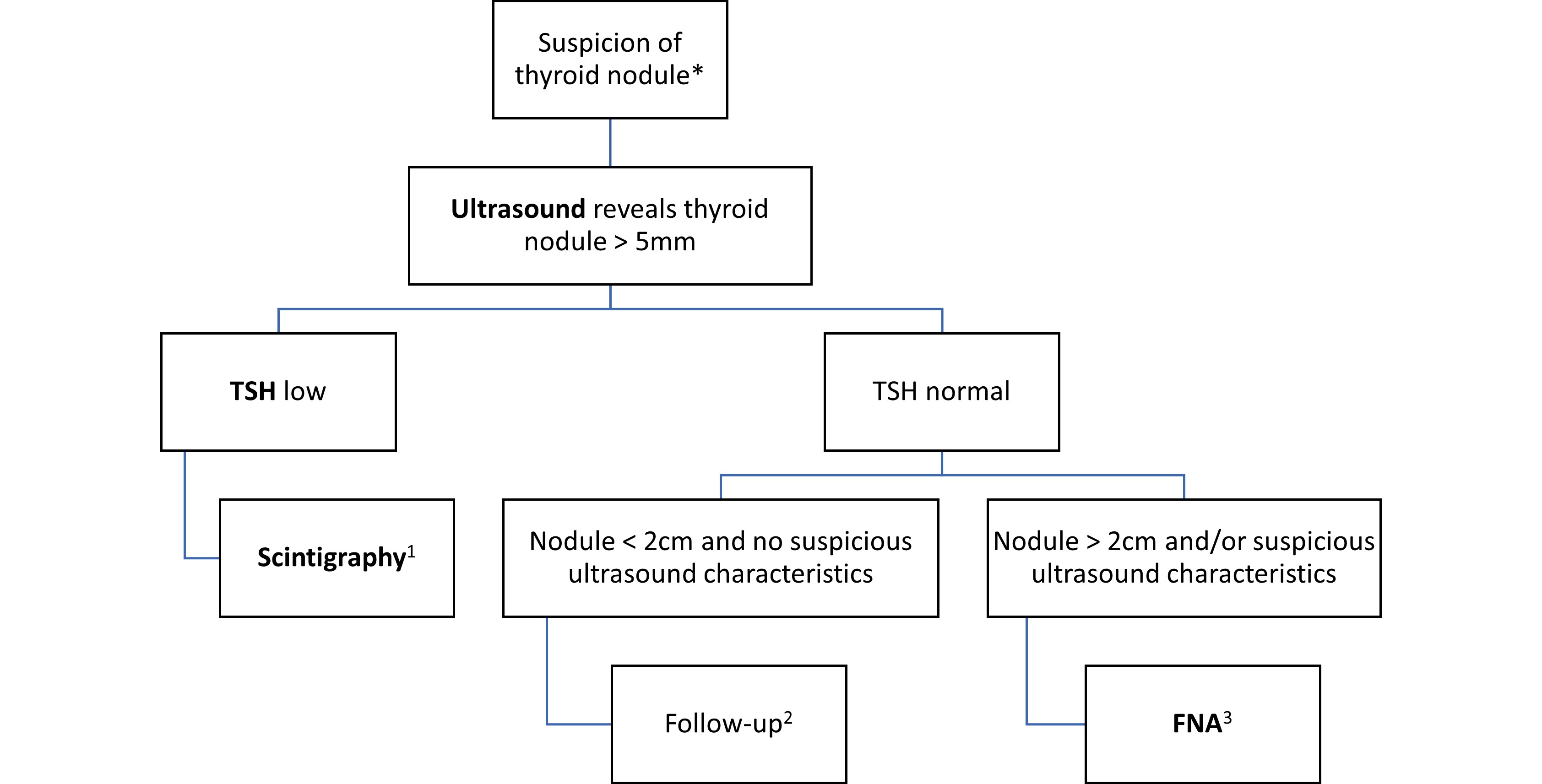
There are basically two purposes of the examination of a patient. On one hand, it is to decide who is in need of surgery (or other definitive therapy), and, on the other hand, it is to determine what needs to be done for patients who do not require surgery. Figure 1 summarizes the algorithm of an evaluation. In more than 95% of the newly diagnosed patients, TN, all TSH, US, and FNA are enough to get the diagnosis and to determine further steps. |
We have to add the fact though that this is true only under ideal conditions, i.e., when the US is performed by the clinician and FNA is available whenever necessary and FNA is performed by an experienced cytopathologist. Practice shows that if the clinician does not perform the US himself or there is a problem with FNA, often other, otherwise unnecessary examinations will be requested. We have summarized those conditions in Table 1 in which we require other diagnostic tests. |
||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||
WHAT ARE THE MAJOR FEATURES OF THYROID ULTRASOUND EXAMINATION? |
|||||||||||||||||||||||||||||||||||||
US is the basis of the diagnosis of TN and guides further diagnostic steps. Thyroid US is able to detect discrete lesions smaller than 1 mm in maximal diameter. This sensitivity clearly exceeds all other imaging studies and had inevitably led to a poor specificity regarding not only malignant tumors but even the diagnosis of pathological nodules. We have no objective tools to separate discrete lesions which are not pathological nodules from those that are. Thyroid US has a crucial role in all three indications of surgery. In autonomously functioning adenomas, the role of US is to detect the nodule. US is the only diagnostic test which is able to measure both the size of the nodule and often more importantly the size of the nodular lobe. Therefore, US has a decisive role in the surgical indication of goiters causing compression signs. Measuring the nodule(s) and the thyroid lobes is the basis for the follow-up of those patients who do not require operation at an actual examination but can be candidates for surgery later in their lifetime, if their thyroids grow. An US report that does not include |
the three diameters of the nodule(s) and diameters of the thyroid lobes is not suitable for this purpose. There is a well-established role of US in guiding FNA, and it is expected that sampling should be US-guided. While in the last decade of the twentieth century, the guiding principle was to recognize all malignant thyroid lesions, the trends in the last decade, the principle has been changing, with an increasing effort to avoid FNA for benign thyroid lesions. Although there are quite a few features that can be used to find a statistically significant difference in the US presentation of benign and malignant nodules, several things are always worth considering. Firstly, these characteristics have a great role in papillary thyroid cancers but fail in the recognition of follicular carcinomas. The latter is more prevalent in iodine-deficient countries compared with iodine-replete areas. Secondly, there is no biological standard regarding most suspicious characteristics, and therefore the interobserver agreement ranges only from fair to moderate in the judgment of these features. |
||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||
In order to come to a conclusion based on these features, it inevitably leads to some of the malignancies not being recognized. We can minimize the risk to overlook clinically relevant malignancies, but the risk will be never zero, especially in the case of follicular carcinomas. There is no universal cost-benefit calculation; this varies greatly from country to country. The published guidelines reflect the economical and healthcare conditions of rich countries which, additionally, are iodine-replete countries. Finally, while we make a tremendous effort to reduce |
cytological demand, it may be even more important to reduce the rate of unnecessary US examinations. A rationally composed US report has great importance (see Table 2). Archiving the video taken during the US examination can be a significant help in terms of both a surgery and the comparison required for subsequent examinations and quality assurance. Capturing some images for these roles cannot fulfill these requirements. |
||||||||||||||||||||||||||||||||||||
WHAT IS THE TIRADS CLASSIFICATION? |
|||||||||||||||||||||||||||||||||||||
Thyroid imaging reporting and data systems have been published by all important thyroid associations in the last several years. They categorize thyroid nodules based |
on the risk of malignancy and serve both for comparison of results among different evaluation groups and for indication on FNA (see Table 3). |
||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||
WHAT IS THE ROLE OF ASPIRATION CYTOLOGY? |
|||||||||||||||||||||||||||||||||||||
FNA is the key to distinguish between benign and malignant thyroid lesions. For indication of FNA, see Table 1. This is a test that is easy to perform and also an inconvenience for the patient by being a blood test. On the other hand, the thyroid gland is one of the most difficult organs because general cytological signs suggesting the presence of a tumor (e.g., atypia, pleomorphism) are much less useful in the thyroid gland than in other organs because hormonal influences and thyroiditis might have greater impact on the presentation of thyroid cells than malignant transformation. |
As the main limitation, FNA is not able to discriminate between the most frequent thyroid tumor, the follicular adenoma, and its malignant counterpart, the follicular carcinoma. As a consequence of the abovementioned obstacles, with a very good sensitivity (95-98%), the specificity and positive predictive value of the method is around 60% for a highly experienced thyroid cytopathologist. |
||||||||||||||||||||||||||||||||||||
WHAT KIND OF CLASSIFICATION SYSTEMS ARE USED FOR THYROID CYTOLOGY? |
|||||||||||||||||||||||||||||||||||||
| Although the Bethesda system became very popular in the last 15 years, older and more established reporting systems can also be used (see Table 4). The former has the advantage first of all for less experienced cytopathologists, because with the introduction of category III (atypia or follicular proliferation of unknown significance), we are not forced to make decisions beyond our capabilities and/or beyond the limitations of the technique for certain patterns. Irrespectively of the reporting system used, the cytological finding should be expected to be clear and suitable for deciding what to do next. While the Bethesda system seems to lead to a |
better communication among cytopathologists and clinicians, paradoxically, the introduction of Bethesda system has further strengthened a traditional and occasionally not very efficient approach: Members of the evaluation teams communicate only after they have concluded their reports. This is in striking contrast with the histopathology: A histopathologist is aware of all clinical and radiological findings, which may have influenced her/his pathological report. Such approach in cytology, i.e., the consideration of US features before the FNA diagnosis, might have an even more influential role. |
||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||
WHEN TO PERFORM THYROID SCINTIGRAPHY? |
|||||||||||||||||||||||||||||||||||||
| The role and therefore the use of scintigraphy have substantially decreased by introducing FNA and US in the evaluation. Thyroid scintigraphy (99m Technetium (Tc) pertechnetate or 123-I) must be performed in patients who would be candidates for radioiodine therapy, i.e., in those with undetectable TSH level and nodule >1 cm otherwise not requiring surgery. Thyroid scintigraphy might have a role in the case of |
euthyroid patients in whom FNA raises the suspicion of a follicular tumor: By detecting autonomously functioning adenoma, the patient can avoid surgery. These are those situations in which scintigraphy influenced the decision if all other circumstances of the evaluation are ideal - including the provision of regular follow-up examinations, as well. |
||||||||||||||||||||||||||||||||||||
THE ROLE OF MOLECULAR BIOLOGY IN THE EVALUATION OF NODULAR GOITER PATIENTS |
|||||||||||||||||||||||||||||||||||||
| While these techniques have a constantly increasing role in the prognosis of malignant thyroid tumors, currently they have limited role in the diagnosis and differential diagnostics of TN. One of the major concerns in the evaluation of TN is the lack of preoperative tools in discrimination of benign and malignant follicular tumors. The issue is much more complex as there is a significant difference in the histological separation of follicular adenoma and follicular carcinoma even among highly experienced physicians. |
Novel molecular techniques including mutation analysis of genes involved in thyroid cancer pathogenesis (e.g., RAS, BRAF, PTEN, TERT, RET/PTC), molecular classification based on mRNA (messenger RNA) expression (transcriptome), and microRNA expression analysis show promising results in the differentiation of benign and malignant thyroid tumors. |
||||||||||||||||||||||||||||||||||||
WHAT ARE THE BASIC CONSIDERATIONS ABOUT THYROID SURGERY? |
|||||||||||||||||||||||||||||||||||||
The accepted methods of surgery are (near) total lobectomy or (near) total thyroidectomy. The traditional subtotal resection is not accepted as the risk of having to operate on the same lobe again in the event of a recurrent nodule must be ruled out. In the case of an experienced thyroid |
surgeon, the risk of both permanent recurrent nerve damage and permanent hypoparathyroidism is less than 1% after the first surgical procedures, and it is ten times higher if the patient has to have repeated surgery on the same lobe. |
||||||||||||||||||||||||||||||||||||
WHAT ARE THE INDICATIONS FOR SURGERY AND NONSURGICAL TREATMENT? |
|||||||||||||||||||||||||||||||||||||
The indications of a definitive treatment are enlisted in Table 5. These states in detail are the following. |
|||||||||||||||||||||||||||||||||||||
Low TSH level |
|||||||||||||||||||||||||||||||||||||
| It is quite clear that persistently undetectable TSH levels, i.e., subclinical (normal FT4/FT3 levels with undetectable TSH) or overt (elevated FT4 and/or FT3 levels) hyperthyroidism, are cardiological risk factors and therefore require definitive therapy. |
There is a gray zone when the TSH is detectable but below the lower limit. This can coexist with nonautonomously functioning nodules in a person with either an otherwise healthy thyroid gland or an autoimmune thyroid disease. Subsequent follow-up examinations in these borderline cases will decide what to do exactly. |
||||||||||||||||||||||||||||||||||||
Surgical indication based on the results of FNA |
|||||||||||||||||||||||||||||||||||||
| There is no doubt that a patient with suspicious (Bethesda V) or malignant (Bethesda VI) FNA report requires surgical intervention. The issue is the follicular proliferation, categorized either as Bethesda III (follicular lesion) or Bethesda IV (follicular tumor or suspicion of follicular tumor). In these patients we have to consider other factors as well, including the size and the US presentation of the lesion and the affected lobe and also the age and wish of the patient. |
Hopefully, molecular techniques will add some new insights to this issue in the near future. It is very important that there is no worldwide uniform cancer incidence in these two categories. These incidences have to be determined in each evaluation group. In such cases, regular US and FNA monitoring of the patient may be considered instead of surgery. |
||||||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||||||
Compression caused by enlargement of the thyroid gland |
|||||||||||||||||||||||||||||||||||||
| While there is little probability for uncertainty in the case of low TSH and suspicious FNA, the third reason for surgery can be determined with much more uncertainty. From a practical point of view, it is very important that it is not the size of the nodule but the size of the nodular lobe that determines whether the nodule causes any compression symptoms. There is a close relationship between thyroid size and body weight, and the location of the thyroid has also a great influence. |
The lower the thyroid gland, the smaller the enlargement can cause compression and vice versa. It is clear that the patient's age significantly influences the decision, as well. The prognosis and therefore our proposal are different in a significant but not yet surgical case at age 20 and age 80. We also need to mention the important fact that a neck complaint of compression may not be caused by a (thyroid) disease. |
||||||||||||||||||||||||||||||||||||
WHAT KIND OF OTHER INDICATIONS FOR DEFINITIVE THERAPY CAN BE ESTABLISHED? |
|||||||||||||||||||||||||||||||||||||
| The patient's wish is the most important that has to be taken into account when the reasons above do not apply to the case. If the nodule is visible and esthetically disturbs the patient, it must be accepted that the patient wants to have surgery. |
A significant proportion of patients have difficulty tolerating the awareness that there is a so-called abnormal, albeit invisible, lesion in their thyroid gland. In that case, it needs to be explained even more thoroughly to the patient that the risk of having surgery is clearly greater than if it is not done. |
||||||||||||||||||||||||||||||||||||
| Similarly, it is not uncommon for a physician experienced in the thyroid gland to believe that a tumor may exist despite a negative FNA finding. This happens in two scenarios. One is when there is data suggesting the possibility of a tumor: a suspicious palpation finding, vocal cord paralysis unexplained by other reasons, a rapid growth of a solid nodule, and a nodule that |
appears particularly suspicious on an US. The other situation is encountered when FNA is repeatedly nondiagnostic for a solid nodule. 5-10% of all cytological examinations fall into this category even for highly experienced teams. |
||||||||||||||||||||||||||||||||||||
| A special situation is for benign cysts that recur even in the case of repeated aspiration, which can be treated by alcohol treatment with very good results. |
However, it must be taken into account that alcoholic treatment as well as surgery in the case of cysts that do not cause complaints and do not exceed 2-2.5 cm can rarely be professionally justified. |
||||||||||||||||||||||||||||||||||||
THE ROLE OF RADIOIODINE THERAPY |
|||||||||||||||||||||||||||||||||||||
| Radioiodine therapy (RAI) is the preferred treatment of autonomously functioning autonomous adenomas either solitary or multifocal when the patient became clinically or subclinically hyperthyroid. RAI of euthyroid patients is not justified except for large autonomous adenomas because such patients frequently remain euthyroid even for their entire lifetime. |
The gray zone is the subnormal TSH, i.e., when TSH is detectable but it is below the normal range: RAI should be considered if the thyroid worsens the patient's cardiac status. Large-dose RAI is also used for decreasing large, nontoxic multinodular goiters when surgery is contraindicated. |
||||||||||||||||||||||||||||||||||||
THE ROLE OF NONSURGICAL THERAPIES IN THE TREATMENT OF THYROID NODULES |
|||||||||||||||||||||||||||||||||||||
| Percutaneous ethanol sclerotherapy, thermal ablation with radiofrequency or laser, microwave ablation, and high-intensity focused US are the possible alternatives for surgery. In contrast with other alternatives, ethanol sclerotherapy is very cheap and easy-to-perform and is the only modality in which we have gained long-term (>10 years) follow-up data on the efficiency. It has a well-established role in recurrent thyroid cysts. Any of the nonsurgical methods might have great role in special circumstances |
by decreasing the size of a benign nodule at least temporarily. Patients with high risk of anesthesia or surgical complications (recurrent nodules) and pregnant women are the main candidates. We have to consider in other patients that the risk of thyroid surgery is very low, and surgery is much more efficient than any of the alternatives. Moreover, it is not justified to treat a patient without surgical indication with nonsurgical interventions. |
||||||||||||||||||||||||||||||||||||
WHAT TO DO IN PATIENTS WHO DO NOT NEED DEFINITIVE THERAPY? |
|||||||||||||||||||||||||||||||||||||
| Because TN nodule cannot be treated with drugs, the fundamental question is whether any of the conditions described in detail earlier will develop that will require surgery later in the patient's lifetime. This is almost always due to the growth of the lobe containing nodule(s). Repeated US and TSH in 1 to 3 years is the usual approach in euthyroid patients. The smaller the nodule, the longer the interval of follow-up examination. |
We did not anticipate that a benign nodule is able to become malignant; however, we have to consider the 5-10% false negative rate of FNA. Therefore, in nodules which increase by more than 30% in volume, FNA should be repeated. The bases of the follow-up are the size of the nodular lobe and that of the nodule(s). That is why it is crucial to give the three diameters of them at the first and subsequent US examinations. |
||||||||||||||||||||||||||||||||||||
CONCLUSIONS |
|||||||||||||||||||||||||||||||||||||
Those who have the possibility of a nodular goiter should be examined on the basis of palpation, neck complaints, or patient history. US screening is not justified as a starting point as that would inevitably place an unmanageable burden on the examination system and US screening occasionally leads to unnecessary surgeries. The US examiner has a pivotal role in managing patients with TN. It is in the interest of the patient and the evaluation system to ensure a complete examination with as little load and appearance |
as possible. The key to this is for the clinician to perform both the US examination and the US-guided sampling. It must be ensured that the cytological analysis is performed by a cytologist experienced in thyroid cases. The most common cause of surgery is not the size of a nodule but the enlargement of the lobe containing the nodule. Accordingly, there is no more important data in the US report than the size of the lobes. |
||||||||||||||||||||||||||||||||||||
References
- Gharib, H., Papini, E., Valcavi, R., Baskin, H.J., Crescenzi, A., Dottorini, M.E., Duick, D.S., Guglielmi, R., Hamilton, C.R. Jr, Zeiger. M.A., Zini, M.; AACE/AME Task Force on Thyroid Nodules.: American Association of Clinical Endocrinologists and Associazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocrine Practice 2006 12 63-102.
- Cheung K, Roman SA, Wang TS, Walker HD, Sosa JA. Calcitonin measurement in the evaluation of thyroid nodules in the United States: a cost-effectiveness and decision analysis. J Clin Endocrinol Metab. 2008;93:2173-80. https://doi.org/10.1210/jc.2007-2496.
- Cibas ES, Ali SZ, Conference NCITFSotS. The Bethesda system for reporting thyroid cytopathology. Am J Clin Pathol. 2009;132(5):658-65. https://doi.org/10.1309/AJCPPHLWMI3JV4LA.
- Gharib H, Hegedûs L, Pacella CM. Clinical review: nonsurgical, image-guided, minimally invasive therapy for thyroid nodules. J Clin Endocrinol Metab. 2013;98:3949-57. https://doi.org/10.1210/jc.2013-1806.
- Gharib H, Papini E, Garber JR, Duick DS, Harrell RM, Hegedüs L, Paschke R, Valcavi R, Vitti P. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi Medical guidelines for clinical practice for the diagnosis and management of thyroid nodules - 2016 update. Endocr Pract. 2016;22:622-39. https://doi.org/10.4158/EP161208.GL.
- Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, Schuff KG, Sherman SI, Sosa JA, Steward DL, Tuttle RM, Wartofsky L. 2015 American Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26:1-133. https://doi.org/10.1089/thy.2015.0020.
- Jeh SK, Jung SL, Kim BS, Lee YS. Evaluating the degree of conformity of papillary carcinoma and follicular carcinoma to the reported ultrasonographic findings of malignant thyroid tumor. Korean Journal of Radiology. 2007 May-Jun;8(3):192-197. DOI: 10.3348/kjr.2007.8.3.192.
- Kim SH, Kim BS, Jung SL et al. Ultrasonographic findings of medullary thyroid carcinoma: a comparison with papillary thyroid carcinoma. Korean J Radiol 2009; 10: 101-105.
- Machens A, Holzhausen H-J, Dralle H. The prognostic value of primary tumor size in papillary and follicular thyroid carcinoma. A comparative analysis. Cancer. 2005;103:2269-073. https://doi.org/10.1002/cncr.21055.
- Mauriello C, Marte G, Canfora A, Napolitano S, Pezzolla A, Gambardella C, Tartaglia E, Lanza M, Candela G. Bilateral benign multinodular goiter: what is the adequate surgical therapy? A review of literature. Int J Surg. 2016;28(Suppl 1):7-12. https://doi.org/10.1016/j.ijsu.2015.12.041.
- Nikiforov YE. Molecular diagnostics of thyroid tumors. Arch Pathol Lab Med. 2011;135(5):569-77. https://doi.org/10.1043/2010-0664-RAIR.1.
- Rosai J, DeLellis RA, Carcangiu ML, Frable WJ, Tallini G. (2015) Tumors of the thyroid and parathyroid glands. AFIP Atlas of Tumor Pathology: Series 4: American Registry of Pathology.
- Russ G, Bonnema SJ, Erdogan MF, Durante C, Ngu R, Leenhardt L. European Thyroid Association guidelines for ultrasound malignancy risk stratification of thyroid nodules in adults: the EU-TIRADS. Eur Thyroid J. 2017;6:225-37. https://doi.org/10.1159/000478927.
- Shin JH, Baek JH, Chung J, Ha EJ, Kim JH, Lee YH, Lim HK, Moon WJ, Na DG, Park JS, Choi YJ, Hahn SY, Jeon SJ, Jung SL, Kim DW, Kim EK, Kwak JY, Lee CY, Lee HJ, Lee JH, Lee JH, Lee KH, Park SW, Sung JY, Korean Society of Thyroid Radiology (KSThR) and Korean Society of Radiology. Ultrasonography diagnosis and imaging-based management of thyroid nodules: revised Korean Society of Thyroid Radiology consensus statement and recommendations. Korean J Radiol. 2016;17:370-95. https://doi.org/10.3348/kjr.2016.17.3.370.
- US Preventive Task Force-2017 US Preventive Services Task Force, Bibbins-Domingo, K., Grossman, D. C., Curry, S. J., Barry, M. J., Davidson, K. W., Doubeni, C. A., Epling, J. W., Jr, Kemper, A. R., Krist, A. H., Kurth, A. E., Landefeld, C. S., Mangione, C. M., Phipps, M. G., Silverstein, M., Simon, M. A., Siu, A. L., & Tseng, C. W. (2017). Screening for Thyroid Cancer: US Preventive Services Task Force Recommendation Statement. JAMA , 317 (18), 1882-1887
- Tessler FN, Middleton WD, Grant EG, Hoang JK, Berland LL, Teefey SA, Cronan JJ, Beland MD, Desser TS, Frates MC, Hammers LW, Hamper UM, Langer JE, Reading CC, Scoutt LM, Stavros AT. ACR Thyroid Imaging, Reporting and Data System (TI-RADS): white paper of the ACR TI-RADS Committee. J Am Coll Radiol. 2017;14:587-95. https://doi.org/10.1016/j.jacr.2017.01.046.
- Trimboli, P., Castellana, M., Piccardo, A., Romanelli, F., Grani, G., Giovanella, L., Durante, C.: The ultrasound risk stratification systems for thyroid nodule have been evaluated against papillary carcinoma. A meta-analysis. Rev Endocr Metab Disord 2020 doi: 10.1007/s11154-020-09592-3.
- Tuttle M, Morris LF, Haugen B, Shah J, Sosa JA, Rohren E, Subramaniam RM, Hunt JL, Perrier ND. Thyroid differentiated and anaplastic carcinoma. In: Amin MB, Edge SB, Greene F, Byrd D, Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR, Sullivan DC, Jessup JM, Brierley J, Gaspar LE, Schilsky RL, Balch CM, Winchester DP, Asare EA, Madera M, Gress DM, Meyer LR, editors. AJCC cancer staging manual. 8th ed. New York: Springer International Publishing; 2017.
- www.thyroidmanager.org. Endocrine Education, Inc., Chicago.