
|
|
Lymph nodes in the neck - Case 14.Recurrence of a papillary carcinoma of the thyroid
|
|





Clinical data: a 46-year-old man was referred for evaluation of a lymph node. The patient discovered the node after an upper airway infection for 3 months. The infection lasted 5 days but the node did not change in size thereafter. He was operated on papillary carcinoma for 3 years. Total thyroidectomy and radioiodine therapy was performed. The off-thyroglobulin level increased gradually from 1.9 to 3.1 ng/mL. Radioisotopic evaluation performed off-thyroxine did not reveal any iodine-positive lesions.
Palpation: a firm node above and lateral to the right thyroid.
Functional state: TSH undetectable, FT4 24.7 pM/L on daily 175 microgram levo-tiroxine.
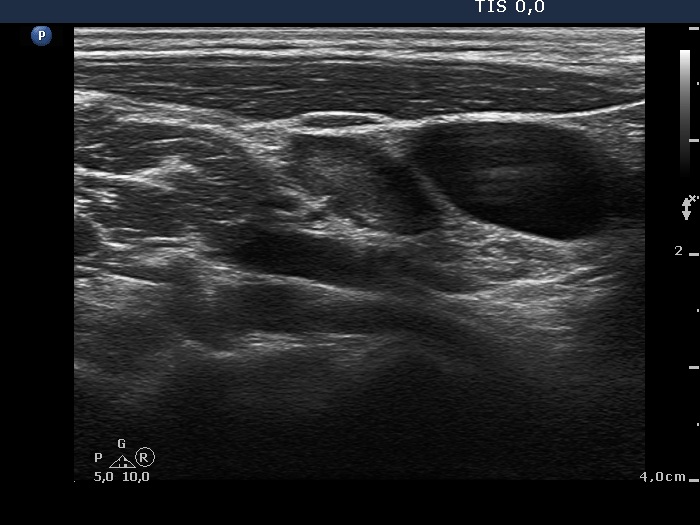
Ultrasonography: there were no thyroid parenchyma in the thyroid beds. A hypoechogenic mass was found at the origin of the right carotid artery. The hilum of the node could not be clearly visualized.
Cytological diagnosis: papillary carcinoma.
Histopathology. The lymph node was removed and a recurrence of a papillary carcinoma to the lymph node was diagnosed. The maximal diameter of the tumor was 4 mm.
Three months after surgery the thyroglobulin level became undetectable and remained so in the next 18 months.
Comments.
-
The presence of an intact hilum is the most important sign of a benign, reactive-type lymph node. However, smaller the size of the node, more frequent the lack of the hilum on ultrasound. It seems likely that in smaller nodes the hilum is located near the capsule of the lymph node and in such cases it is more difficult to identify.
-
The several punctate hyperechogenic granules found in the dorsal part of the node may be either microcalcifications or presentation of fibrosis.