
|
|
Lymph nodes in the neck - Case 15.Extrapulmonary tuberculosis
|
|















Clinical data: a 47-year-old woman was referred us for follow-up investigation. She was examined for two years because of nodular goiter. She noticed a firm painless lump in the left side of the neck for 3 months. She had fatigue and lost 5 kg in weight. Extensive laboratory test were not specific. Thorough examinations revealed a mass in the head of the pancreas suspicious for carcinoma and the lump in the neck was regarded as a metastatic lymph node.
Palpation: there was a not very firm nodule in the right thyroid while a large firm mass in the left side of the neck.
Functional state: euthyroidism (TSH 2.41 mIU/L).
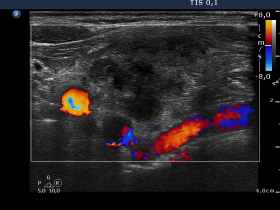
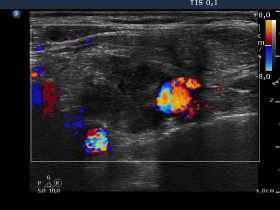
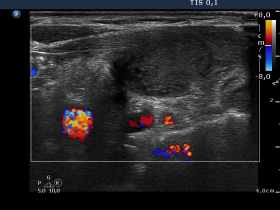
Ultrasonography. There was a moderately hypoechogenic nodule presenting halo sign and perinodular blood flow in the right while two smaller lesions in the left lobe. One of the latter displayed multiple microcalcifications.
The mass in the left side of the neck corresponded to a conglomerate of multiple lymph nodes. These were irregular in shape and presented cystic and necrotic areas. There was no hilum present. The lymph nodes were avascular.
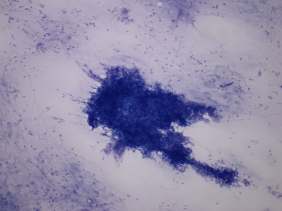
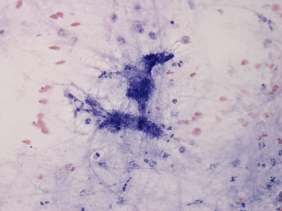
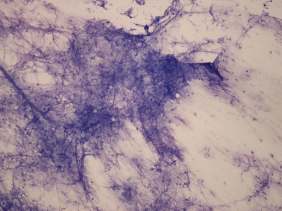
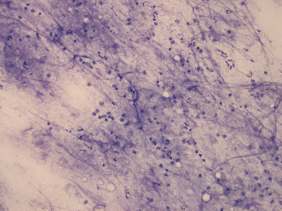
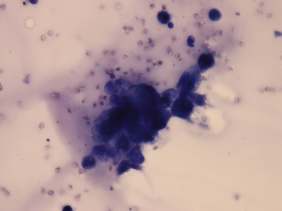
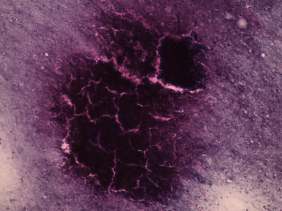
Cytology resulted in benign follicular proliferation, benign colloid goiter and necrosis, right thyroid, left thyroid and conglomerate of lymph nodes, respectively.
The patient underwent on ERCP which excluded pancreatic carcinoma and disclosed necrotic inflammation. A repeat aspiration form the lymph node of the neck was performed in another institute and tuberculosis was diagnosed using PCR assay.
Comment. We did not raise the possibility of extrapulmonary tuberculosis on cytopathology. Our diagnosis was necrotic inflammation, not diagnostic. Nowadays, a necrotic inflammation rarely proves to be tuberculosis but this possibility had to be considered.