
|
|
Papillary carcinoma - Case 47.
|
|

Clinical data: a 45-year-old woman was examined by a cardiologist because of chest pain. She discovered hyperthyroidism and a nodular goiter.
Scintigraphy: the nodule was proved to be a hyperfunctioning nodule. Radioiodine therapy was advised. The patient requested a second opinion.
Palpation: a firm and not freely moveable nodule in the right side of the isthmus.
Functional state: hyperthyroidism (TSH-level undetectable, FT4 28.1 pM/L, FT3 7.17 pM/L).
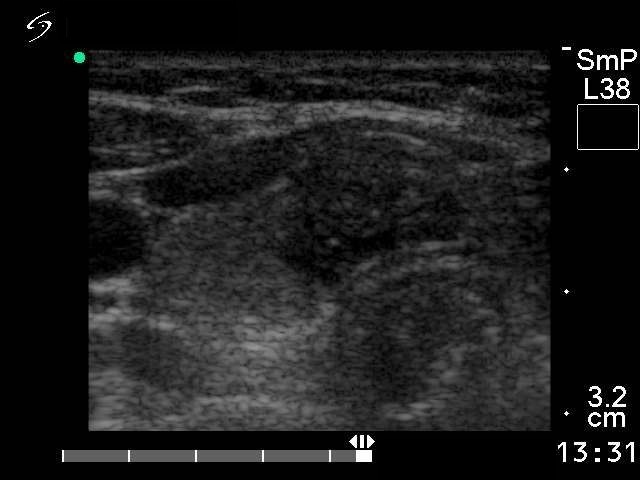
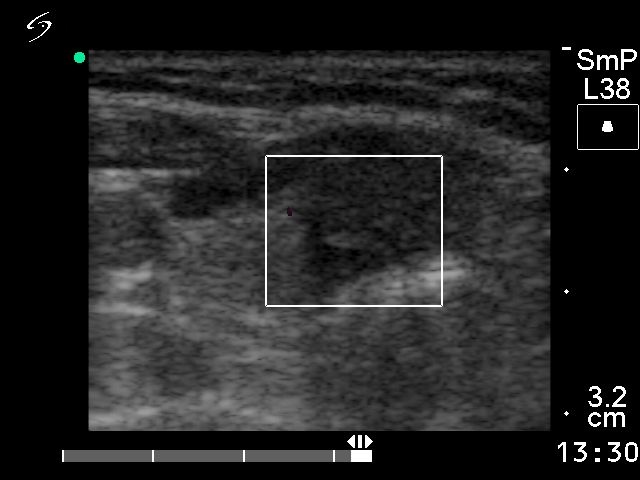
Ultrasonography: a hypoechogenic nodule with microcalcification in the right thyroid. Note the irregular and blurred border of the nodule. The lesion was avascular on Doppler mode.
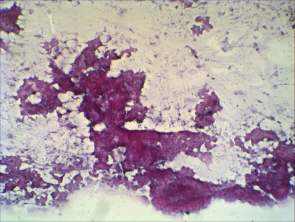
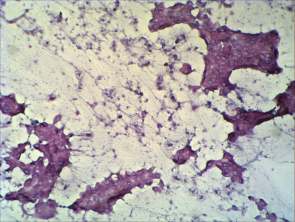
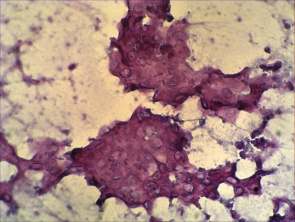
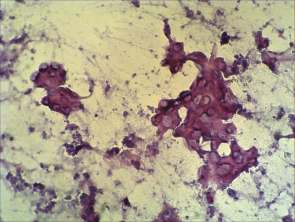
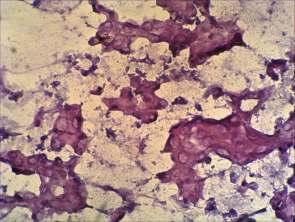
Cytological picture: no colloid in the background. Thyrocytes are arranged exclusively in atypical papillary clusters with nuclear crowding and overlapping. Many pale empty nuclei and grooves can be observed.
Cytological diagnosis: papillary cancer.
Histopathology: papillary cancer (T4N2).
Comment: the main lesson of this case to draw is the importance of the palpation. I had three cases in my practice when a hyperfunctioning nodule as a whole turned to be malignant. (Naturally, in this field papillary microcarcinoma has absolutely no relevance.) In all of these cases, the palpation was the clue to raise the potential oncological significance of the nodule. The US has only limited differential diagnostic potential in this field: both benign toxic nodule and papillary cancer occur in hypoechogenic, inhomogeneous nodule with increased intranodular blood flow. The only sign which has relevance is the blurred border in malignant cases.