
|
|
Benign nodular hyperplasia - Case 3.
|
|









Clinical presentation: A 35-year-old woman was referred for evaluation of a nodular goiter known for years. The thyroid was slowly growing and caused problem in swallowing.
Palpation: The left lobe was enlarged with multiple nodules.
Functional state: euthyroidism with TSH-level 1.06 mIU/L.
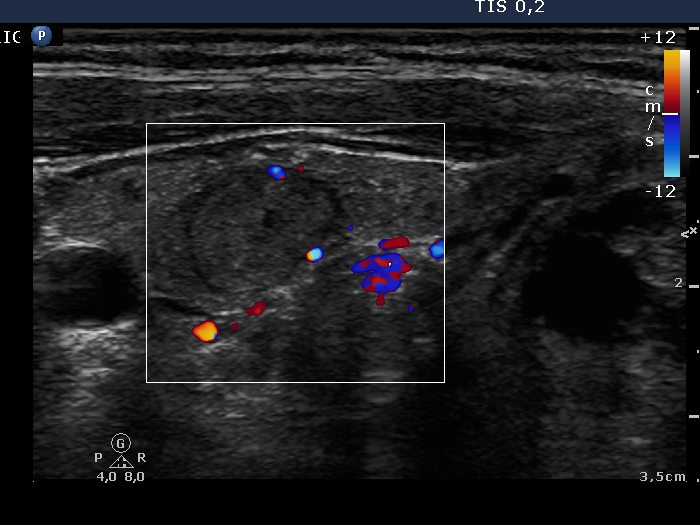
Ultrasonography: The right lobe contained an echonormal nodule, while there were multiple lesions within the left lobe. These were hyperechogenic and presented halo sign and perinodular blood flow.
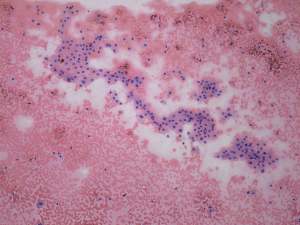
Cytology was performed from the largest hyperechogenic nodule in the left lobe. There was diffuse colloid precipitate in the background. Great proportion of follicular cells exhibited oxyphilic metaplasia. They were located in cohesive groups.
Combined ultrasonographic-cytological diagnosis was benign lesion with great probability: colloid goiter with extensive oxyphilic metaplasia.
The patient was operated on because of the size of the left nodule. The patient wished to be removed her entire thyroid because both her mother and one of her grandmothers previously underwent multiple thyroid surgeries.
Histopathology disclosed benign, hyperplastic nodules in the left lobe while there were no pathological findings in the right lobe.
Comment.
-
This case is an example which demonstrates that the combination of ultrasonographic and cytological data results in better diagnosis than the cytology itself. The cytological pattern can be interpreted either suspicious for oxyphilic tumor or atypia of unknown significance. Considering the sonographic pattern, the lesion is benign with great probability. First, there were multiple nodules with similar echo structure. Second the lack of prominent nucleoli and the lack of dispersed oxyphilic cells argue independently against the possibility of a Hürthle-cell tumor.
A combined clinical-ultrasound-cytological diagnosis would be benign lesion with the risk of malignancy less than 1%. -
The echonormal lesion in the right thyroid is remarkable. It's ultrasound pattern is identical to the non-lesional part of the thyroid. There was no pathological finding corresponding to this lesion.