
|
|
Chronic lymphocytic thyroiditis - Case 50.
|
|




Clinical presentation: a 79-year-old woman requested a second opinion. She was treated for hypothyroidism for more than 15 years. At last investigation in another hospital follicular carcinoma was diagnosed cytologically.
Palpation: the thyroids were firm, no nodule could be palpated.
Functional state: euthyroidism on daily 75 microgram levothyroxine (TSH-level 1.66 mIU/L).
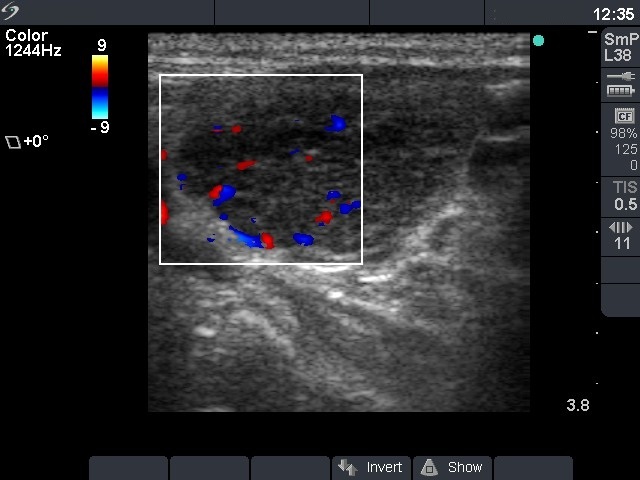
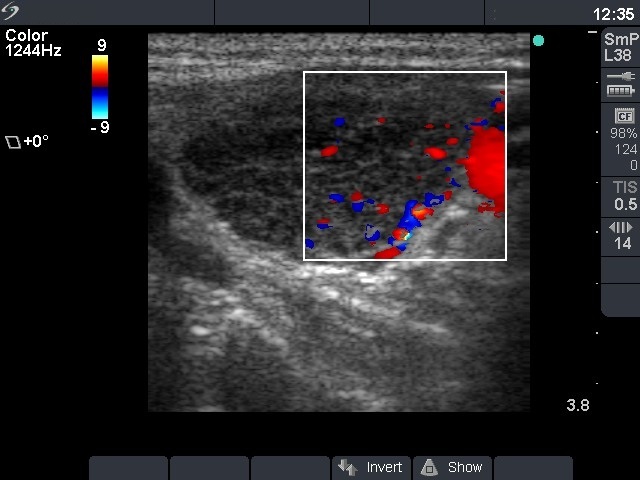
Ultrasonography: the thyroid was minimally hypoechogenic. There were small hypoechogenic areas in the right, while a large nodule-like hypoechogenic lesion with extensive fibrotic changes in the left lobe. The surface of this lesion was irregular. Type 3 vascular pattern was detected, i.e. there was no perinodular blood flow. We could not exclude the possibility that this lesion was a nodule, but the whole pattern was consistent with autoimmune thyroiditis.
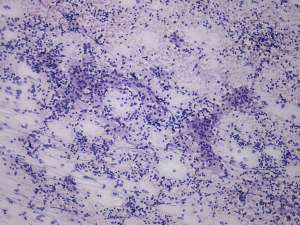
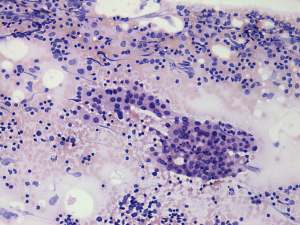
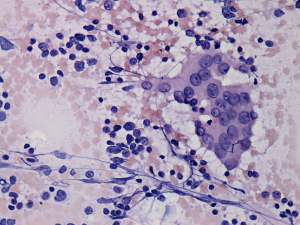
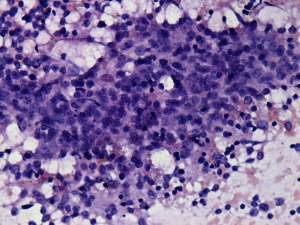
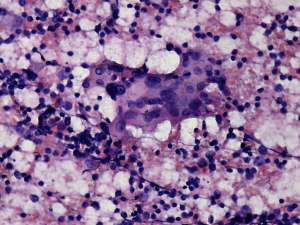
Cytological picture: no colloid in the background. Clusters of Hürthle-cells with heterogeneous lymphoid cells. The atypia of oxyphilic cells was caused by thyroiditis.
Cytological diagnosis: Hashimoto's thyroiditis.
We offered follow-up investigation instead of surgery. The general practitioner advised operation.
Histopathology: Hashimoto's thyroiditis without any nodule.
Comment.
Do not use the term 'nodule' if you have any doubt! A hypothyroid patient must have an autoimmune thyroiditis except for special circumstances (excess iodine intake, painful thyroid, previous radioiodine treatment or surgery). The lack of a halo sign and perinodular blood flow are strong arguments against the possibility of a follicular tumor. We must be aware that in the case of Hashimoto's thyroiditis not only the US pattern but even cytological picture may imitate various other thyroid disorders including a follicular tumor.