Benign cystic areas (ultrasound diagnosis) - case 294 |
|
 |
 |
 |
 |
Essentially, such tiny cystic lesions are normal findings and correspond to dilated macrofollicles.
|
|
|
|
Right lobe |
Left lobe |
 |
 |
 |
 |
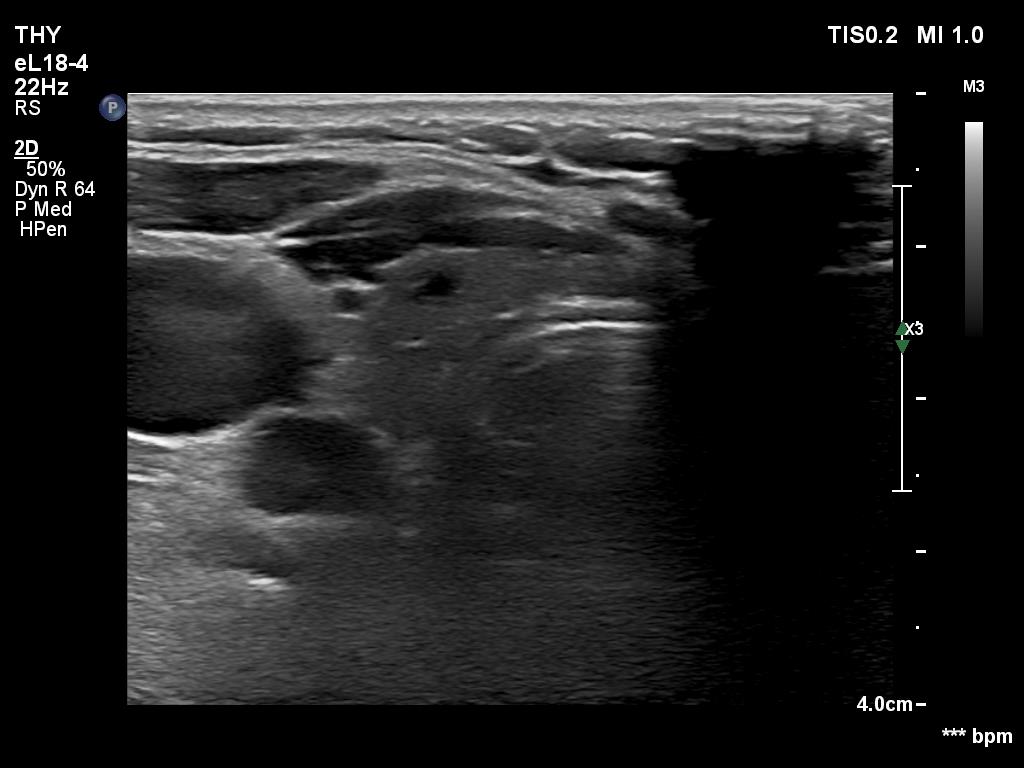
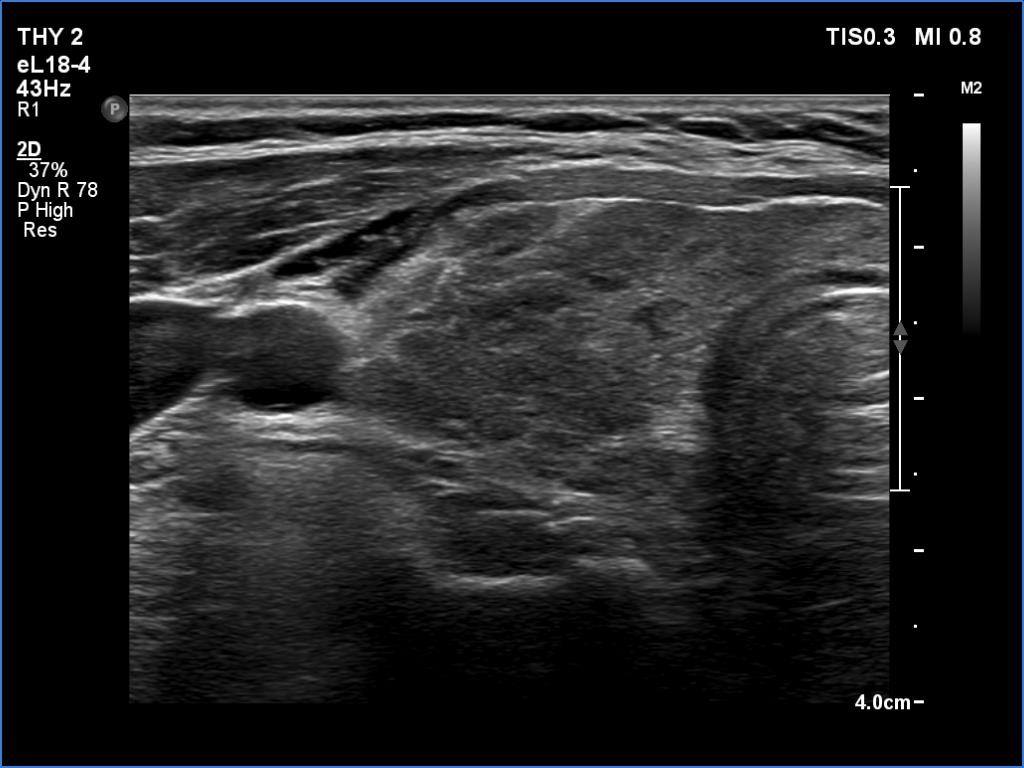
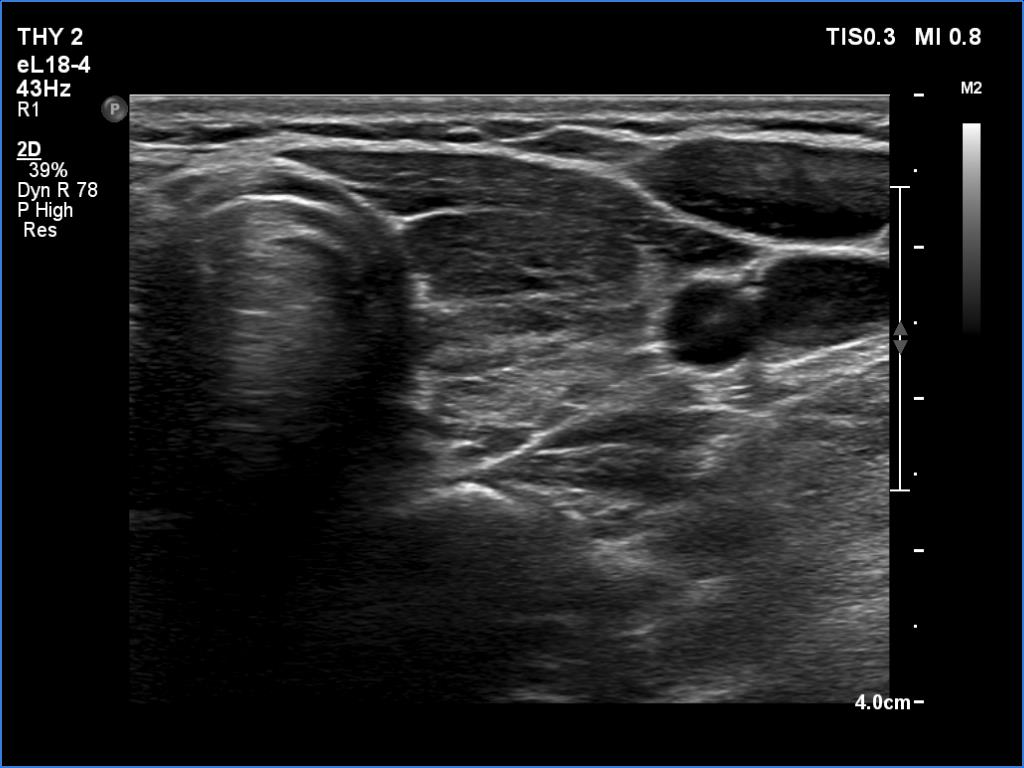
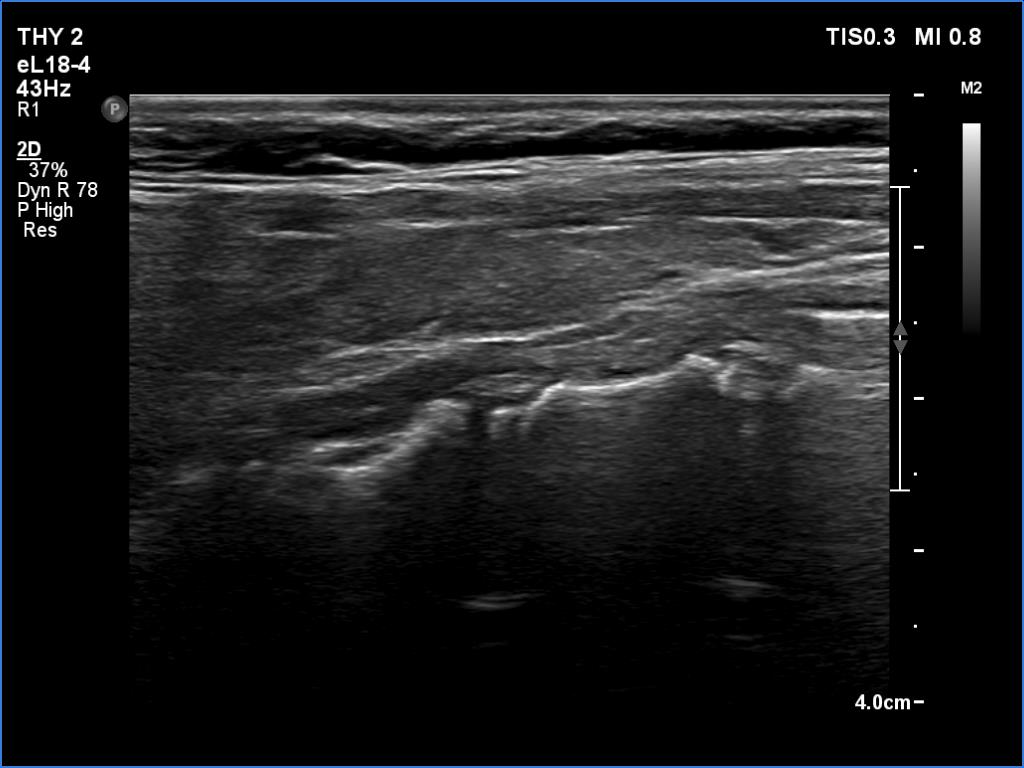
Focal form of lymphocytic thyroiditis is presented. The thyroid has numerous discrete, hypoechoic lesions which correspond to more active foci of thyroiditis. The interpretation of this pattern should not cause concern - these areas are not pathological nodules.
|
|
|
|
Right lobe |
Left lobe |
 |
 |
 |
 |
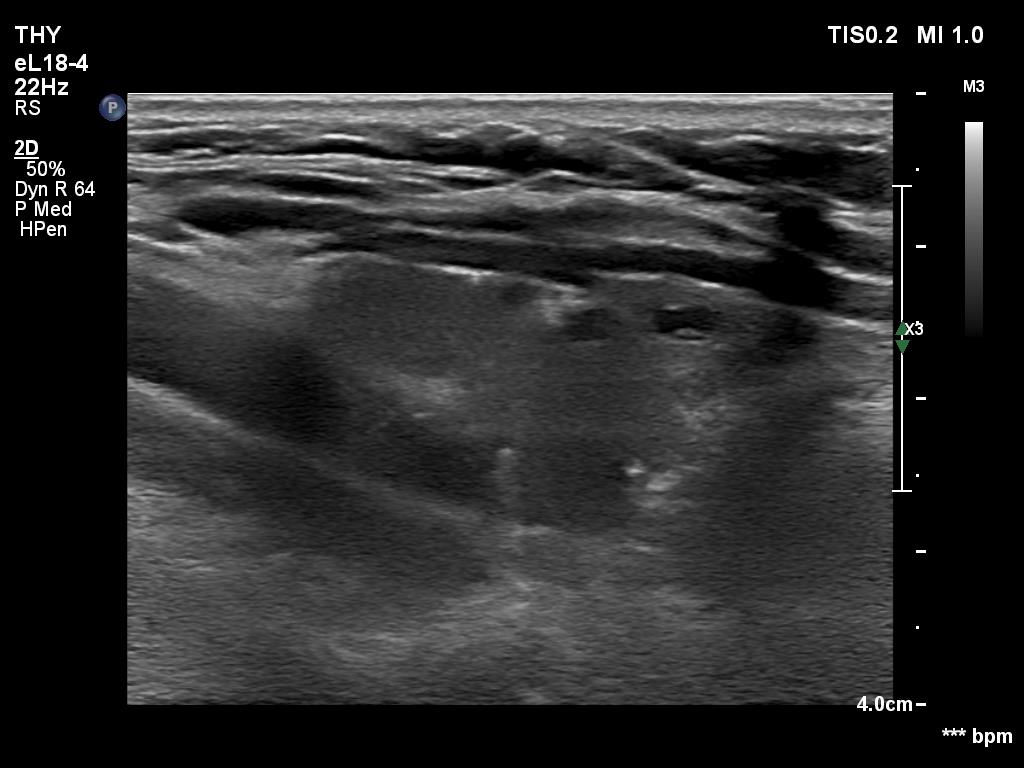
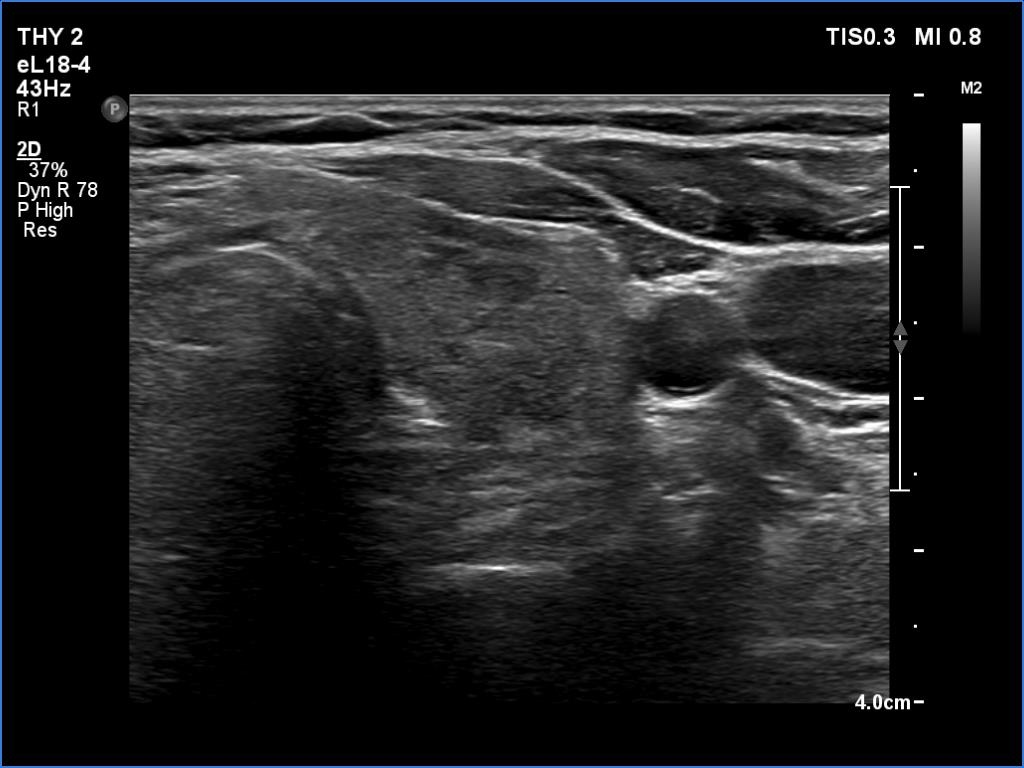
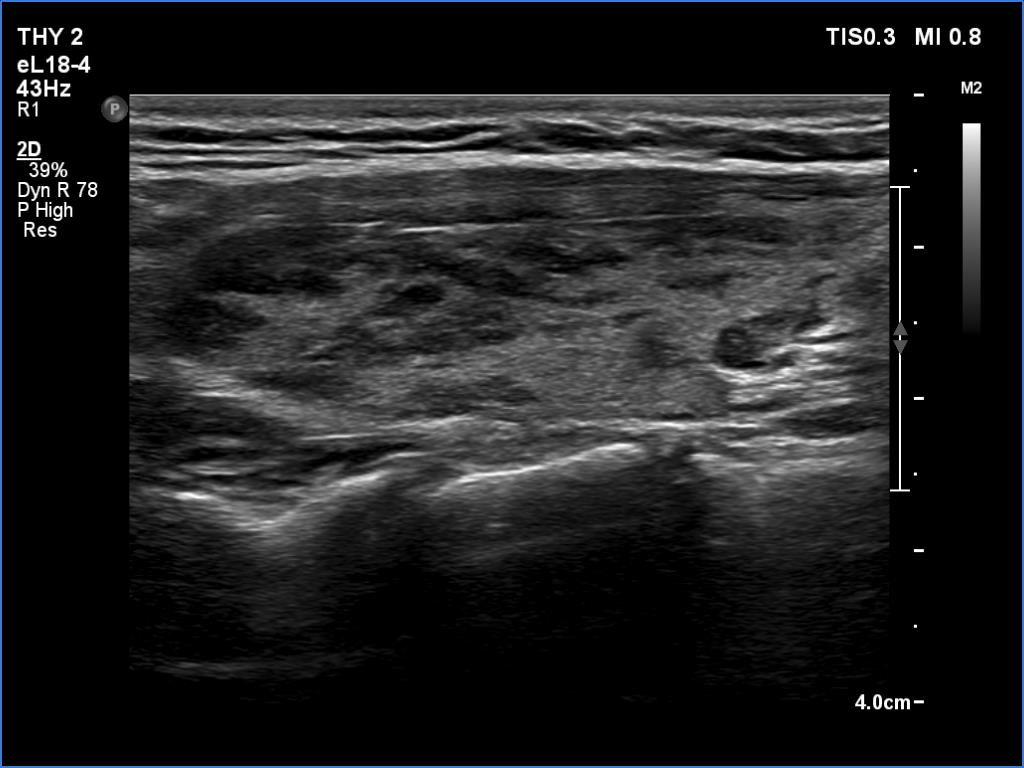
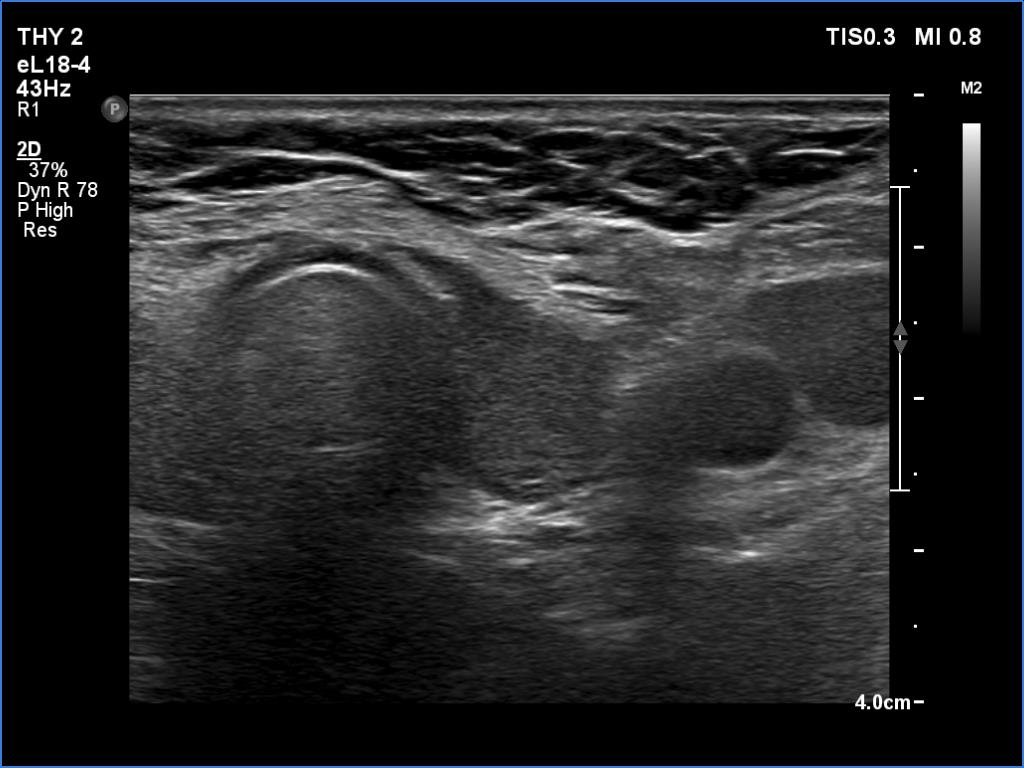
Focal form of lymphocytic thyroiditis is presented. The thyroid has numerous discrete, hypoechoic lesions which correspond to more active foci of thyroiditis. The interpretation of this pattern should not cause concern - these areas are not pathological nodules. The discrete lesions have non-regular, partly clearly lobulated or spiculated margins.
|
|
|
|
Right lobe |
Left lobe |
 |
 |
 |
 |
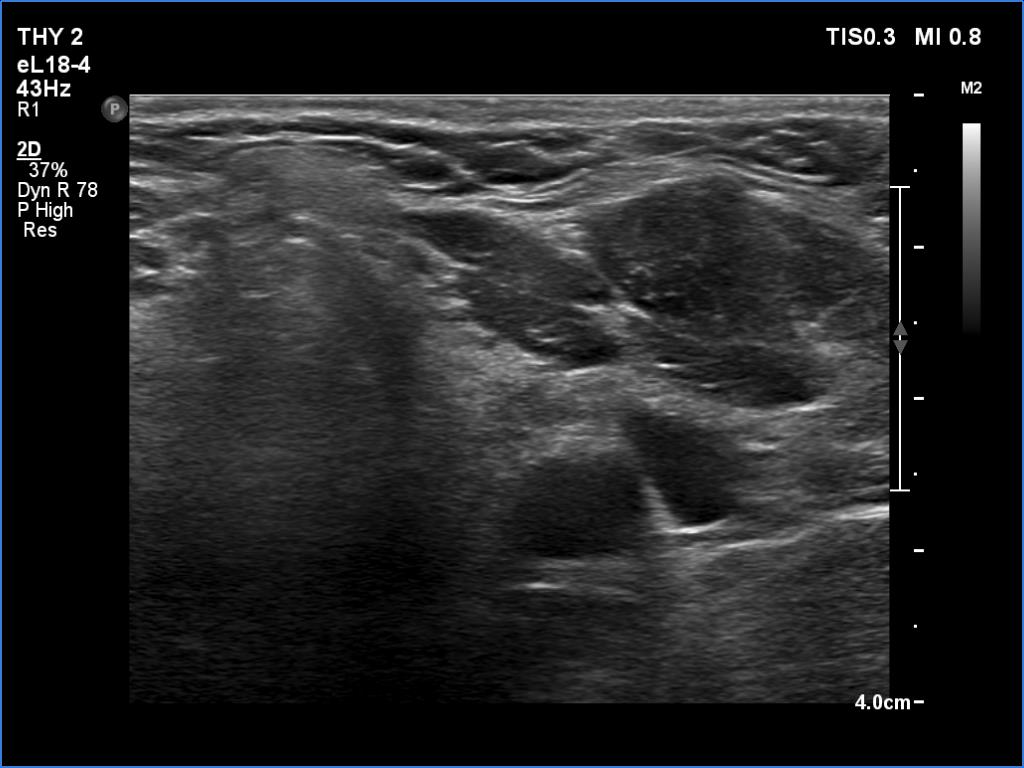
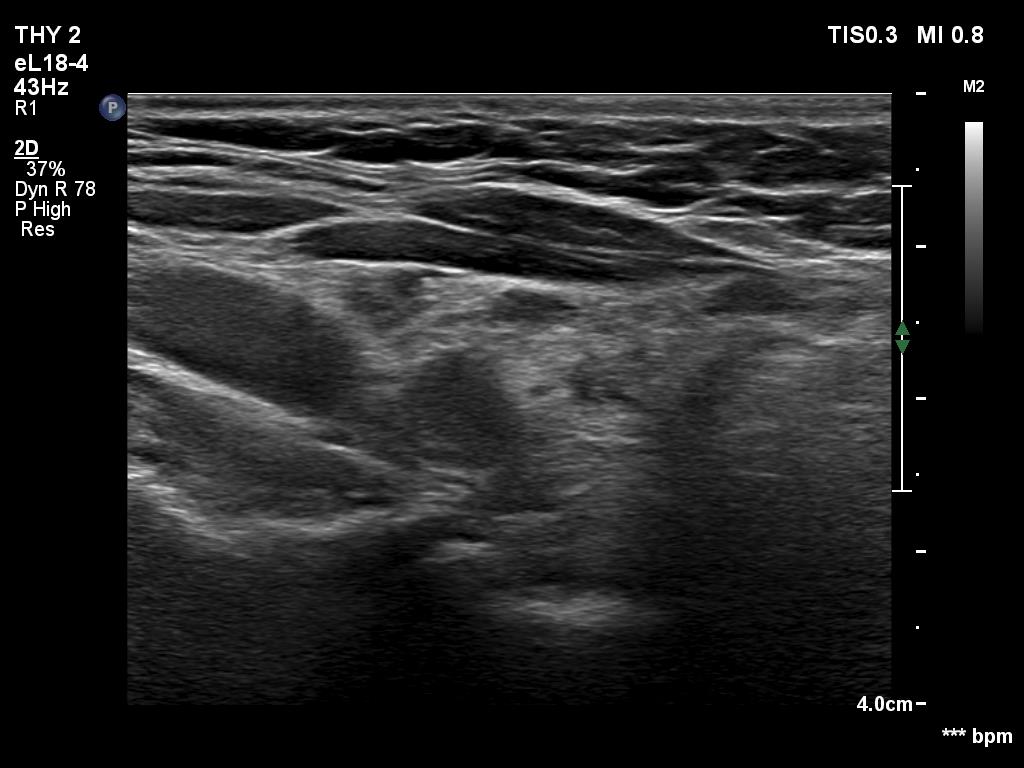
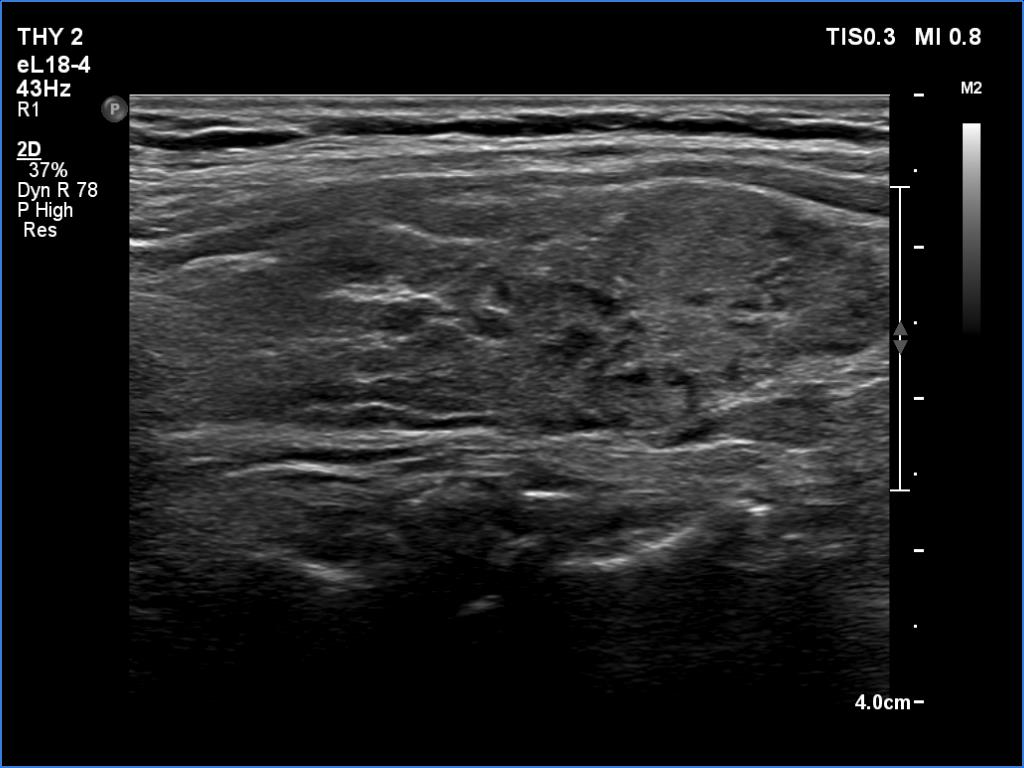
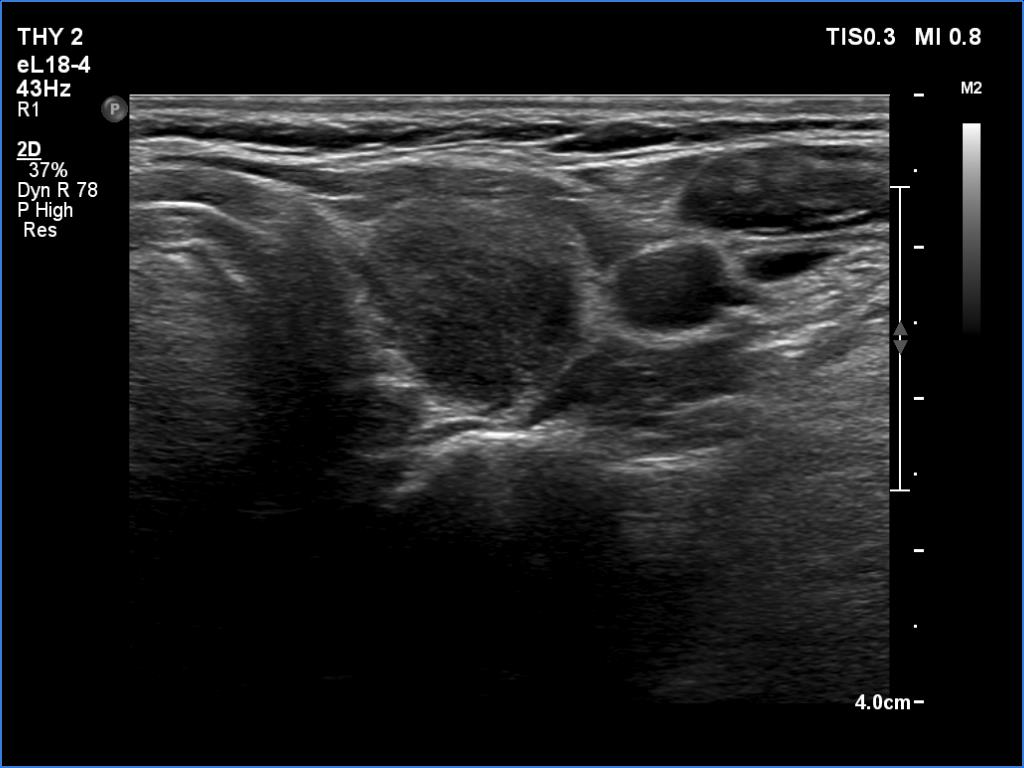
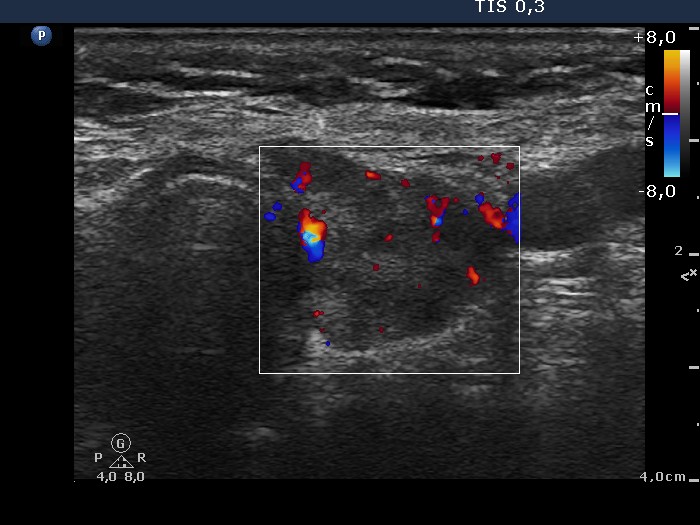
Focal form of lymphocytic thyroiditis is presented. The thyroid has numerous discrete, hypoechoic lesions which correspond to more active foci of thyroiditis. The interpretation of the relatively large ventral hypoechoic area in the left lobe (right upper image can cause problem), however, longitudinal scan decides the issue: this field cannot be a pathological nodule.
|
|
|
|
Examination one |
Six month later |
 |
 |
 |
 |
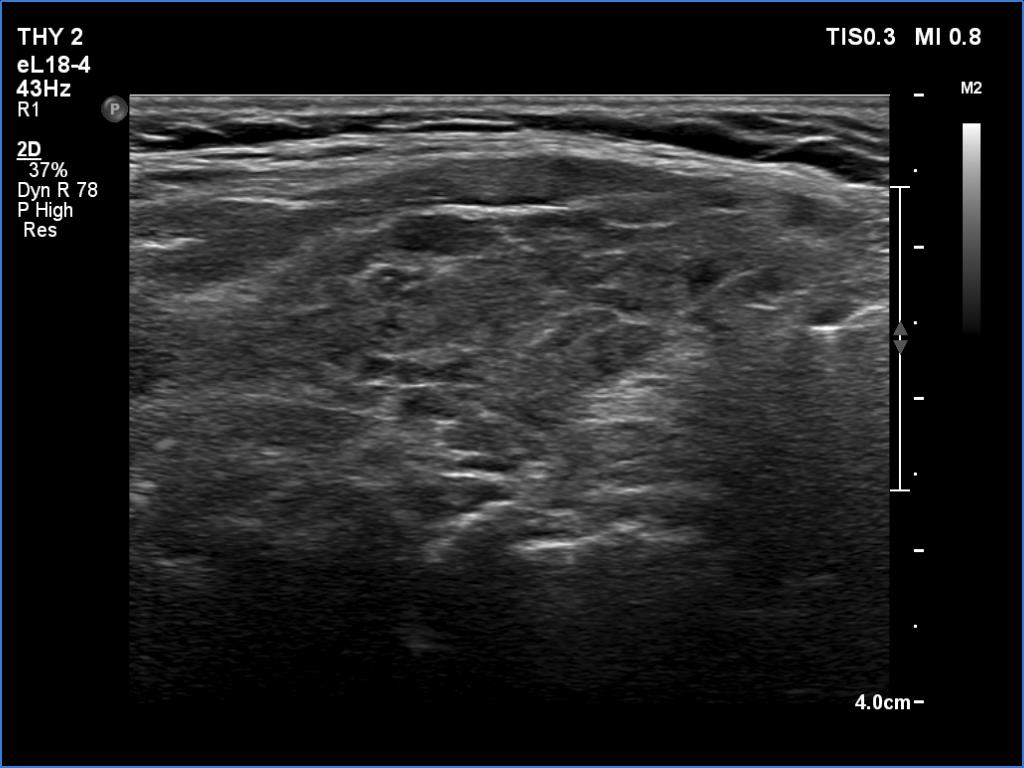
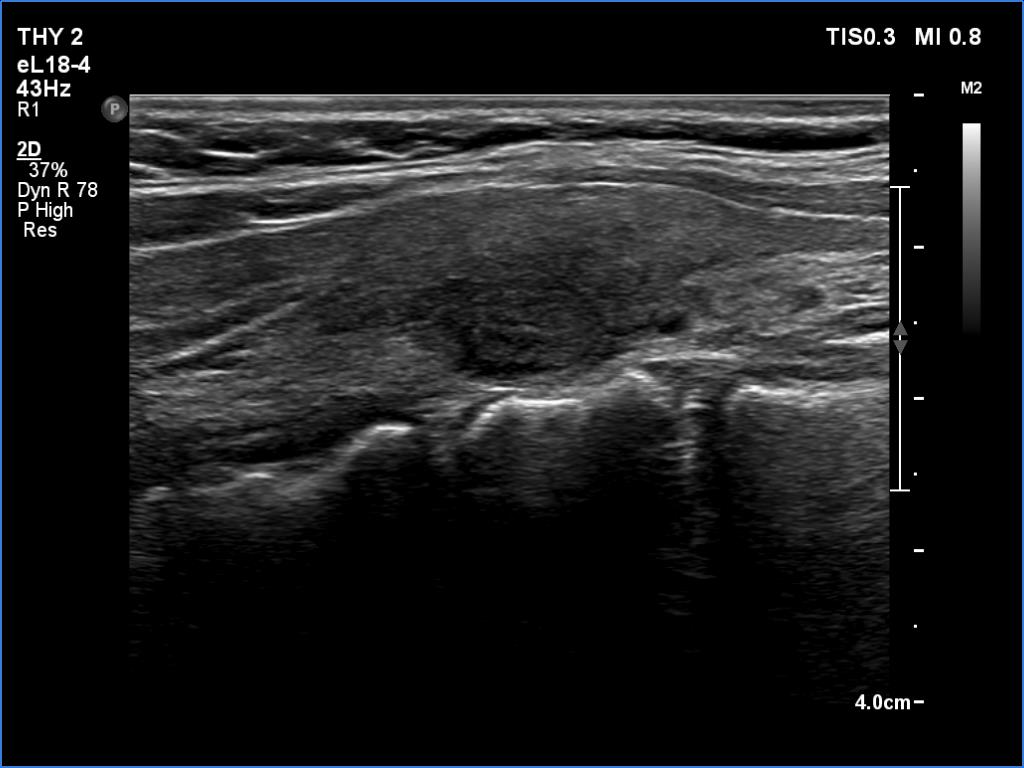
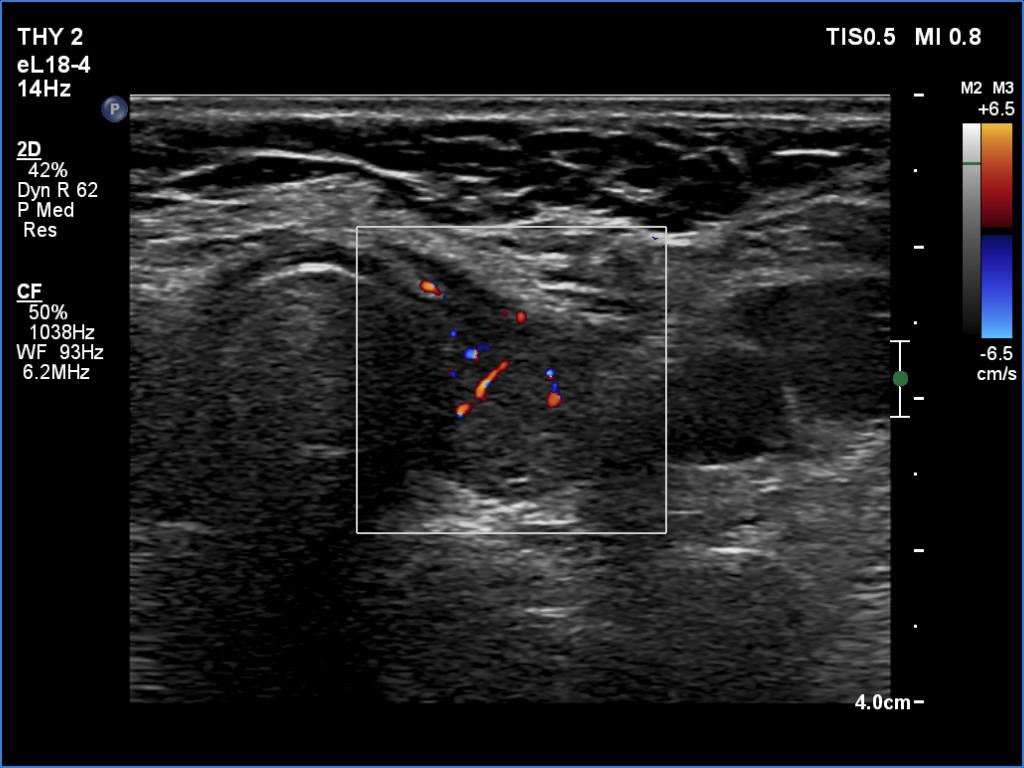
Focal form of lymphocytic thyroiditis is presented. At the first examination, beside smaller hypoechoic areas, the left lobe had a larger discrete lesion. It was doubtful whether this should be regarded as pathological nodule or not. In the first case, the lesion is an EU-TIRADS 5 nodule due to the irregular margins while in the latter, this is an EU-TIRADS 1 lesion. Six months later, the lesion had virtually disappeared which means that this was not a true nodule.
|
| |
|
A patient operated on Graves' disease then received radioiodine therapy - case 321 |
After the surgery before the radioiodine treatment |
After the radioiodine treatment |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
The patient had a recurrent hyperthyroidism 15 years after a bilateral subtotal resection performed because of relapsing Graves disease. Several months after the first visit, the patient underwent on radioiodine treatment. The right images were recorded 5 years after the isotope therapy.
In surgically treated thyroids, the histopathological findings must be taken ito account in order to avoid mispretating discrete lesions. If the previous histopathology did not find nodule than an ambiguous lesion is very rarely a true nodule.
The echonormal areas which surround the hypoechoic lesion can be tracked up, down and sideways, therefore these do not correspond to thyroid tissue but to connective tissue.
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
|
| |
|
|
