
|
|
Case cons100_010
|
|



Clinical presentation: A 59-year-old woman was referred for aspiration cytology. She has been treated for hypothyroidism for two years. A multinodular goiter was found on ultrasound, the nodule in the left lobe did not take up technetium but did MIBI.
Palpation: Both lobes were firm and nodular on palpation.
Functional state: euthyroidism on daily 87.5 microgram levothyroxine (TSH 3.72 mIU/L).
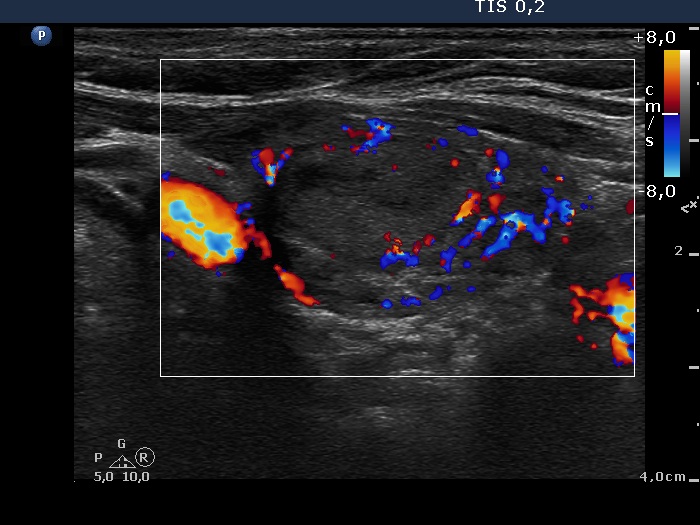
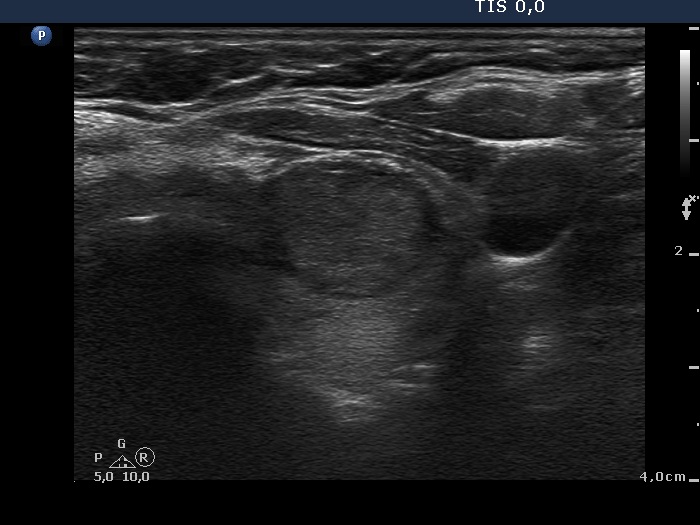
Ultrasonography. The thyroid was moderately hypoechogenic and inhomogeneous. There were multiple echonormal and minimally hypoechogenic discrete lesions in both lobes. Except for the one lesion in the left lobe, these did not correspond to nodule in a pathological sense, while in the event of a minimally hypoechogenic lesion in the left lobe, this possibility could not be excluded.
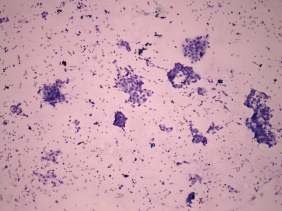
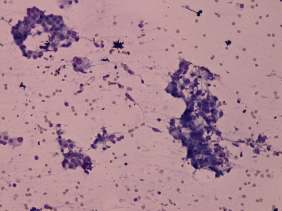
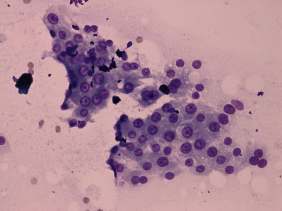
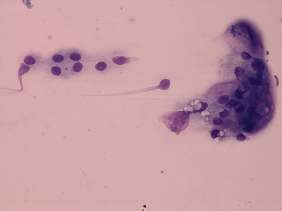
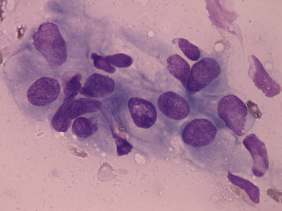
Cytology was performed from the discrete lesion in the left lobe and resulted in Hashimoto's thyroiditis.
Our final diagnosis was hypothyroidism caused by Hashimoto's thyroiditis. A benign lesion in the left lobe.
The patient was sent for surgery by the endocrinologist who initiated the cytology. The reason for the suggestion was MIBI-positivity.
Histopathology disclosed Hashimoto's thyroiditis without any nodule.
Comments.
-
The risk of malignancy in increased if a nodule does not take up radioiodine or technetium but does MIBI.
-
The patient had a deceptive ultrasound presentation on which the possibility of nodules in a pathological sense could not be excluded. It is worth analyzing the ultrasound images and video.