
|
|
Introduction - case 1407
|
|






Clinical presentation: A 63-yr-old woman was referred for a second opinion by her endocrinologist. The patient had a thyroid ultrasound scan a year ago when a nodule was described in her left thyroid lobe. FNA was performed which resulted in oxyphilic variant of a follicular tumor. The endocrinologist had some doubt about the diagnosis.
Palpation: no abnormality.
Laboratory tests: TSH 1.91 mIU/L, aTPO 30 U/mL.
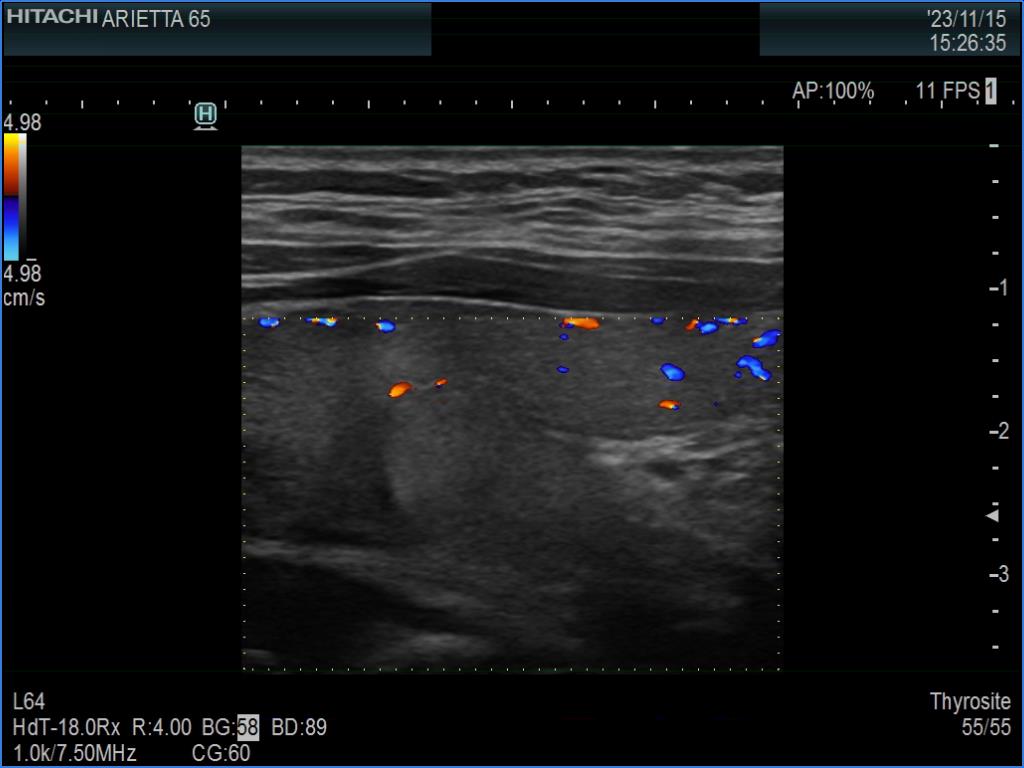
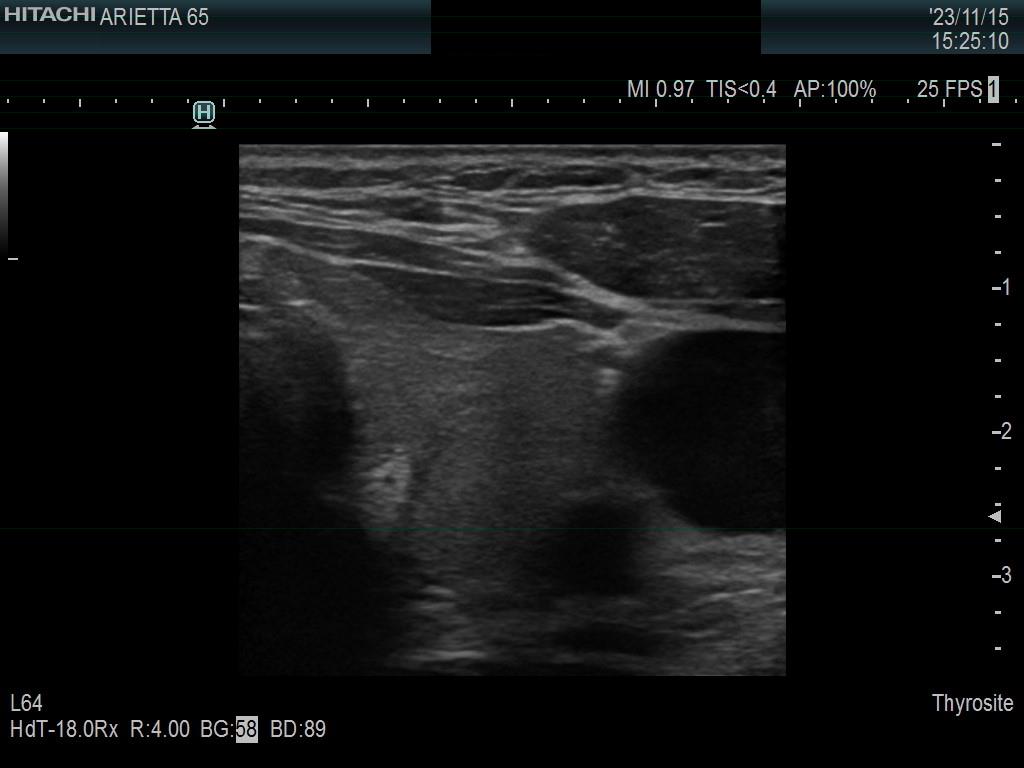
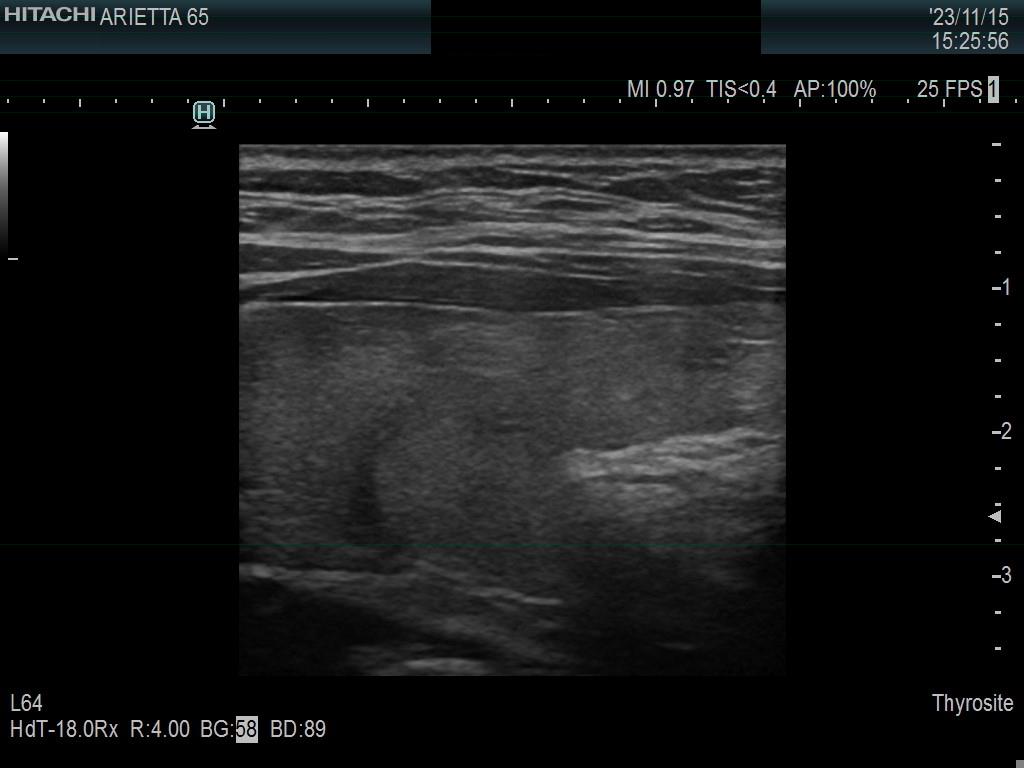
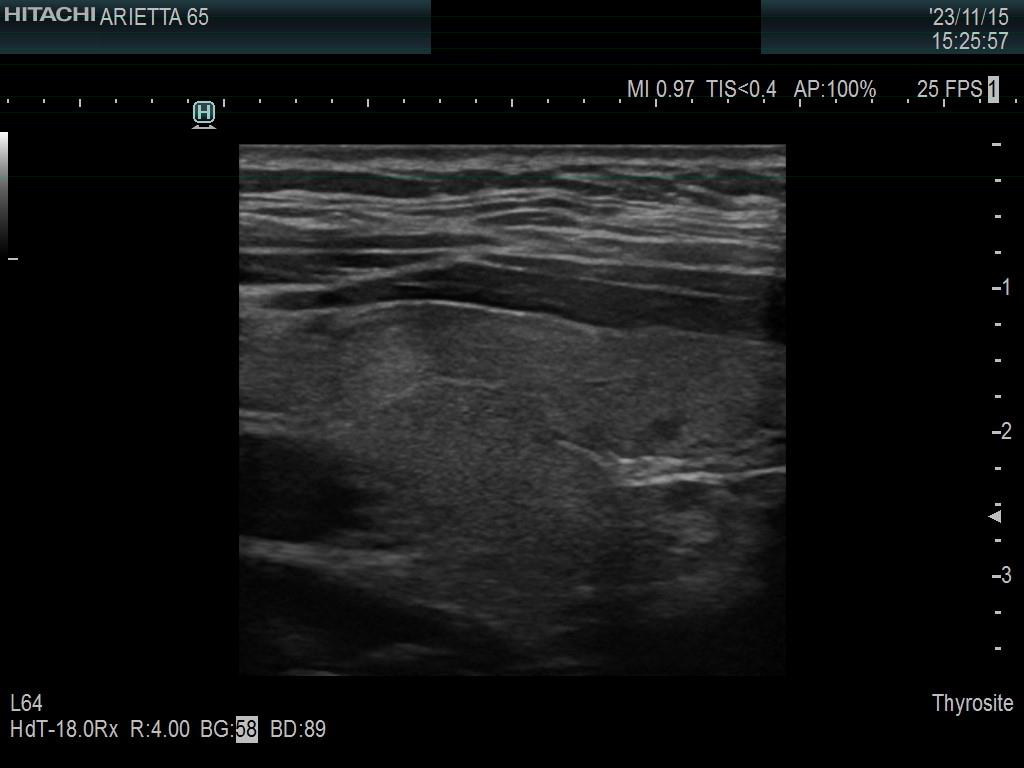
Ultrasonography. The thyroid was minimally hypoechoic. The echogenicity of the dorsal part of the left lobe where the nodule was previously described did not differ from other parts of the thyroid. There was a connective tissue running ventral to this part of the lobe and hypoechoic areas were found upper and dorsal to this. Neither halo nor perinodular blood flow was present.
Suggestion. I did not judge the area as a nodule and suggested ultrasound follow-up instead of surgery. For details of consideration see Comments below.
Comments.
-
The area in question did not correspond to a pathological nodule. It seemed to be circumscribed because of the presence of connective tissue and thyroid vessels.
-
Microfollicular pattern is essential part of a normal thyroid while oxyphilic degeneration is the hallmark of Hashimoto's thyroiditis. The cytological material gained from a Hashimoto's thyroiditis not infrequently mimics oxyphilic variant of a follicular tumor. In the event of a discrete lesion, it is very difficult or even impossible to discriminate a non-tumorous proliferation of follicular cells from an oxyphilic tumor. But in this patient, the lesion from which the FNA was performed was very-very likely not a nodule.
-
A follicular tumor must have a capsule which ultrasound sign, either a complete halo and/or perinodular blood flow are present in more than 95% of cases. Both features were absent in this case.