|
|||||||||||||||||||||||||||||||||
|
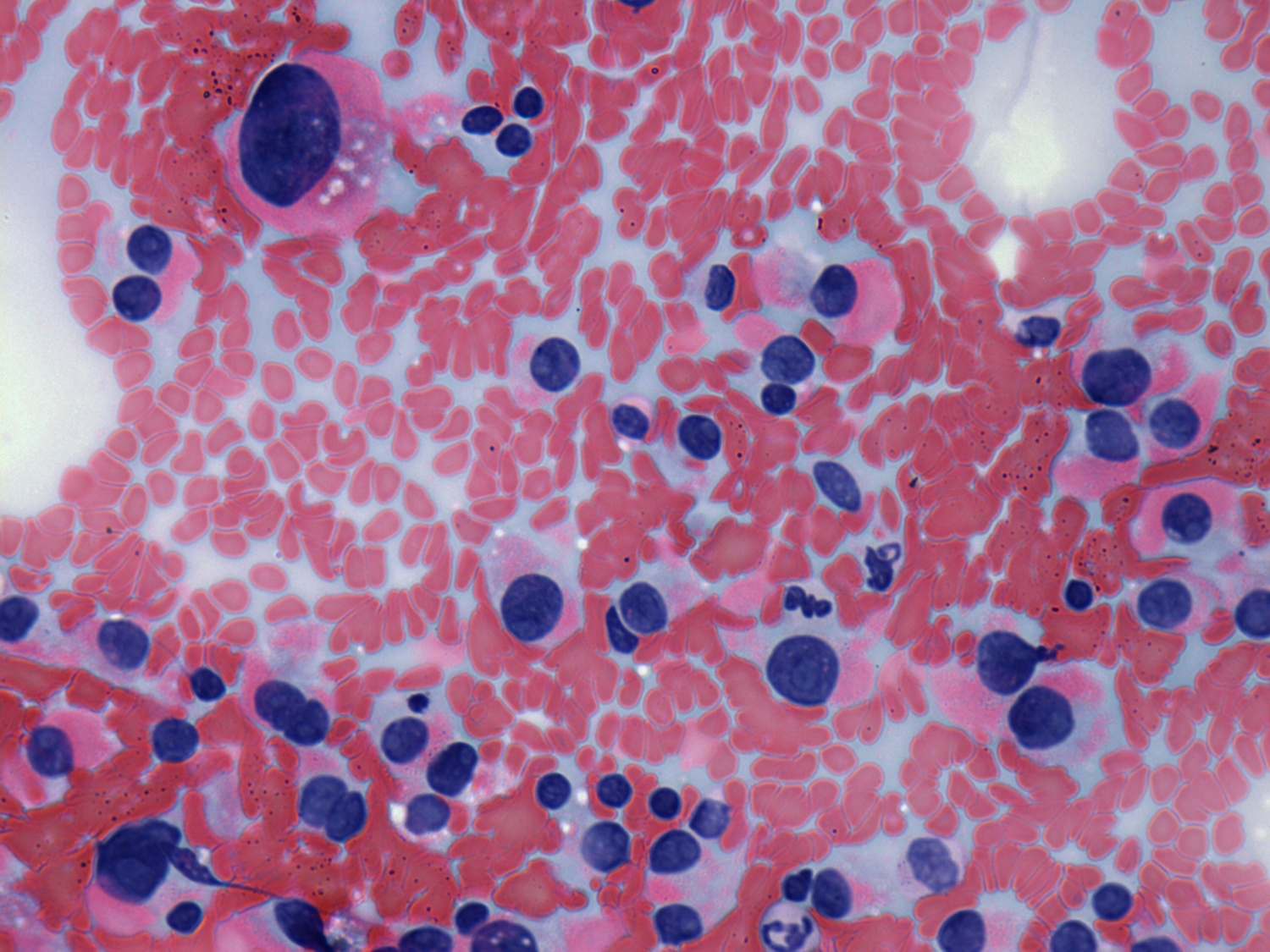
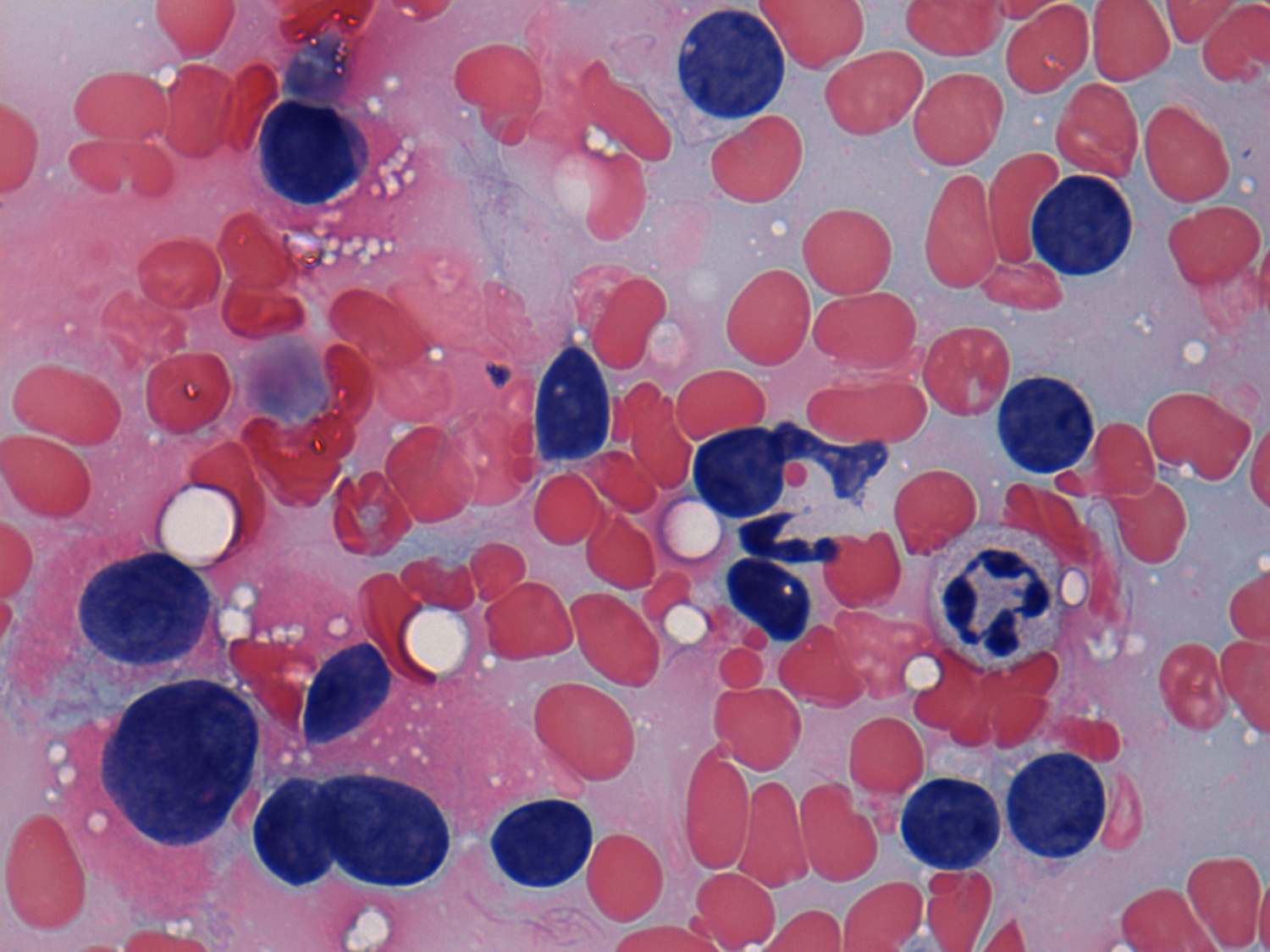
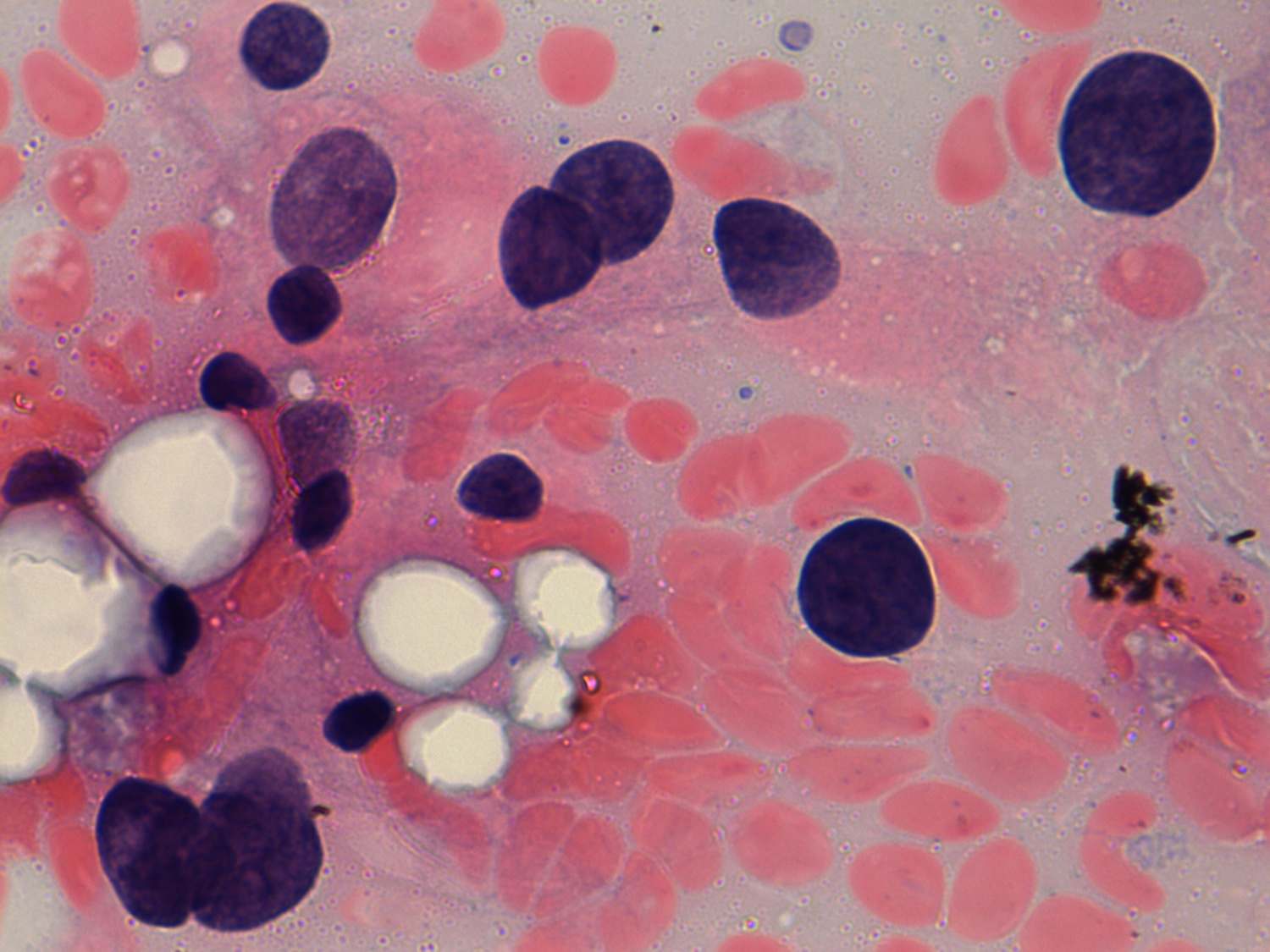
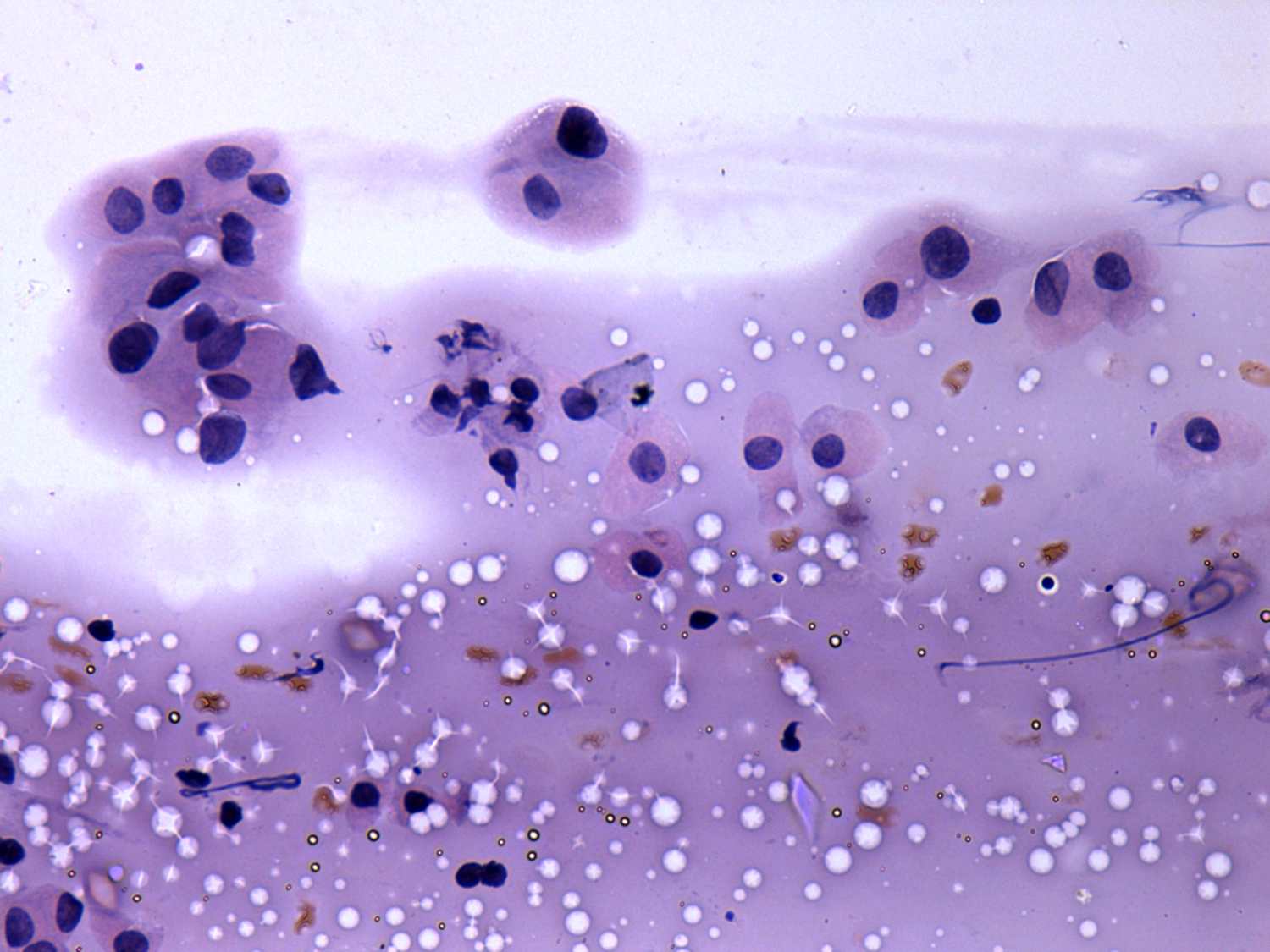
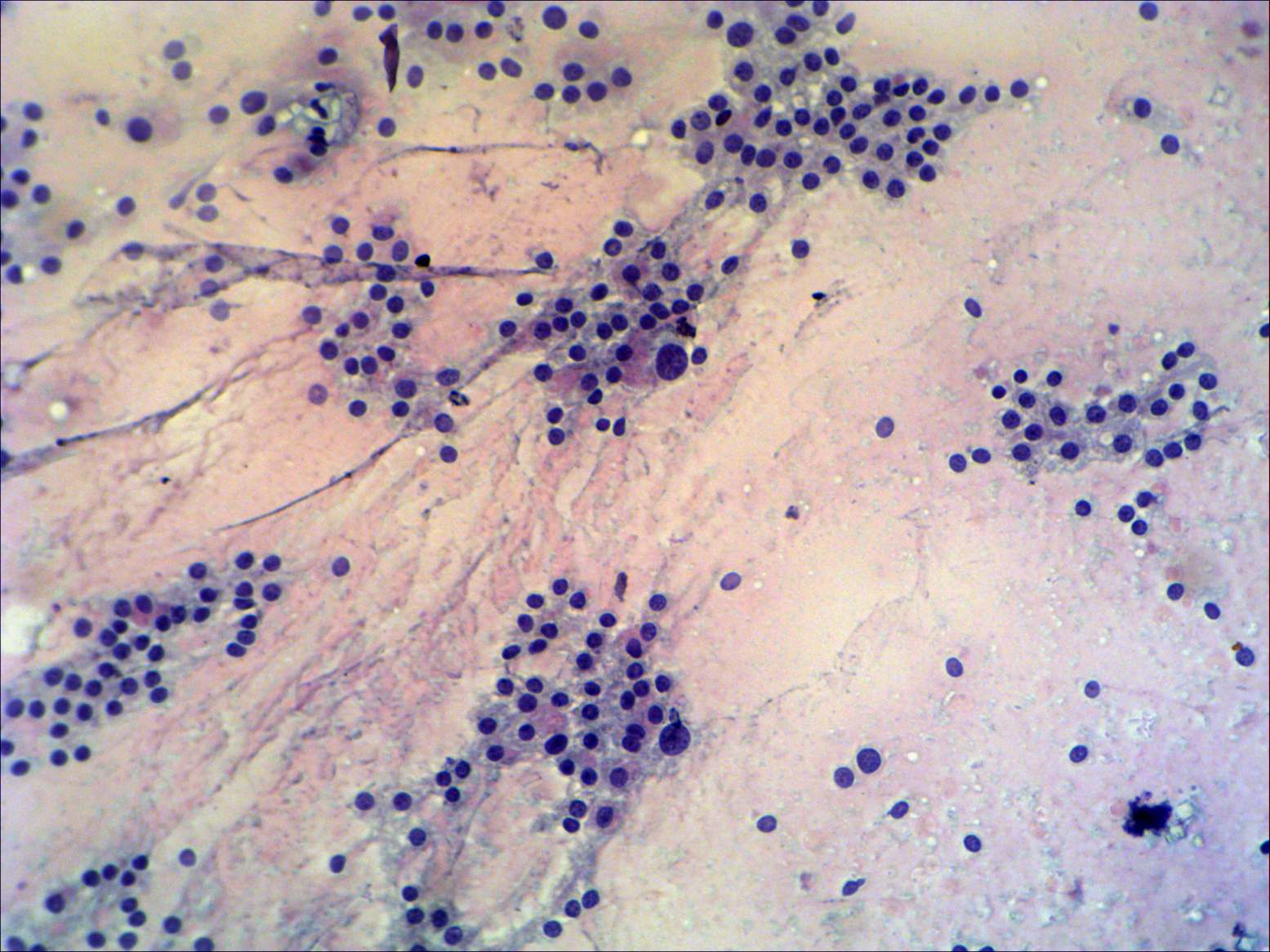
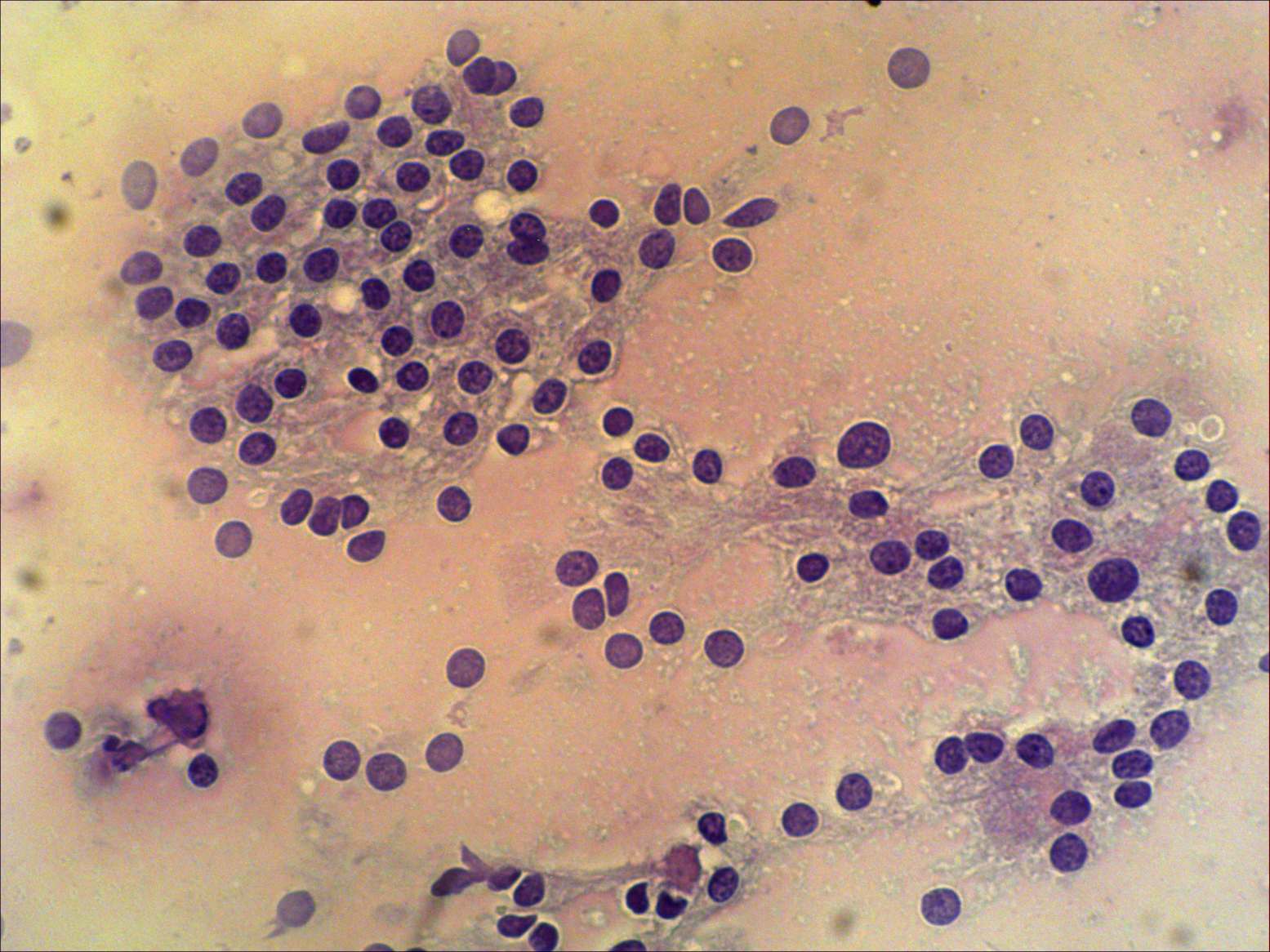
Nuclear enlargement and pleomorphism
|
|||||||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||||||
|
In a hormonally active organ like the
thyroid, the usual signs of nuclear atypia, i.e. anisonucleosis and
pleomorphism has much less relevance than in other organs. The former
has minimal importance in the everyday practice. Moreover, in certain
cases even a monomorphous cellular pattern may raise the possibility of
a follicular tumor.
As regards the latter, it is evident that malignant cells present more frequently pleomorphismism than benign cells. On the other hand, in contrast with many other organs, pleomorphism itself is not enough to give a malignant diagnosis in the thyroid. It is essential to being aware of patient history in order to avoid overdiagnosis of atypical cells. Previous thyrostatic or radioiodine therapy, hormonal influences and first of all oxyphilic metaplasia may cause significant change not only in the size but even in the shape of cells. In certain cases to answer a simple question is enough to reach the goal: which type of malignancy could the atypia that can be seen on the smear belong to? Most if not all cases of papillary cancer presents inclusion or groove. The cellular arrangement in a medullary carcinoma lack follicular formation. As regards cases presenting atypia and microfollicular proliferation, consideration of the sonographic pattern is essential to a correct diagnosis. |
|||||||||||||||||||||||||||||||||