
|
|
Chronic lymphocytic thyroiditis - Case 75.
|
|











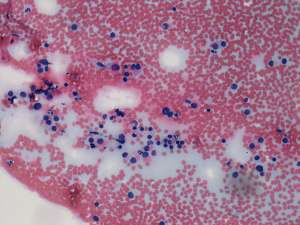
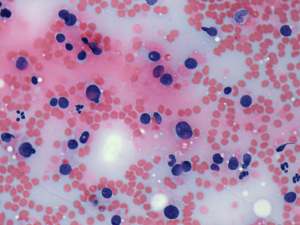

First examination (1st and 2nd rows of images):
Clinical presentation: a 60-year-old hypothyroid patient was referred for an evaluation of a thyroid nodule.
Palpation: the thyroids were moderately firm, a more firm lesion was suspected in the left lobe.
Hormonal investigation indicated euthyroidism on daily 125 microgram levo-tiroxine with TSH-level 0.81 mIU/L.
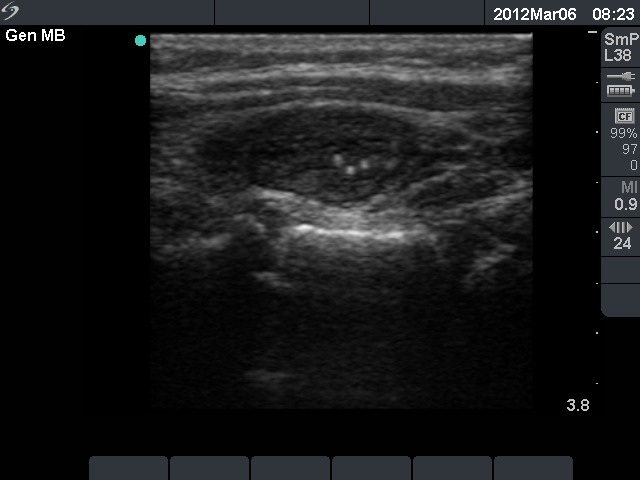
Ultrasonography: the thyroids were moderately hypoechogenic with fibrotic changes. There was a hypoechogenic lesion with microcalcification in the left thyroid.
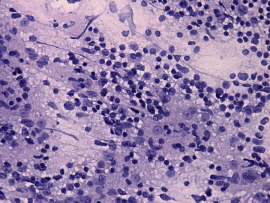
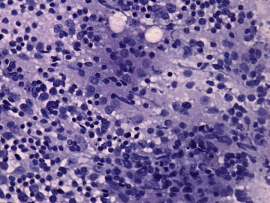
Cytological diagnosis: Hashimoto's thyroiditis.
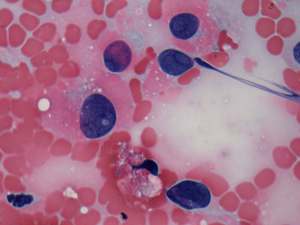
Follow-up examination 2 years later (3rd and 4th rows of images):
Clinical presentation: the patient visited another clinic for follow-up examination. She was told harboring a suspicious nodule and aspiration cytology resulted in suspicion of carcinoma not otherwise specified.
Palpation: a firm nodule was palpable in the left lobe.
Functional state: euthyroidism on daily 125 microgram levo-tiroxine (TSH 2.06 mIU/L).
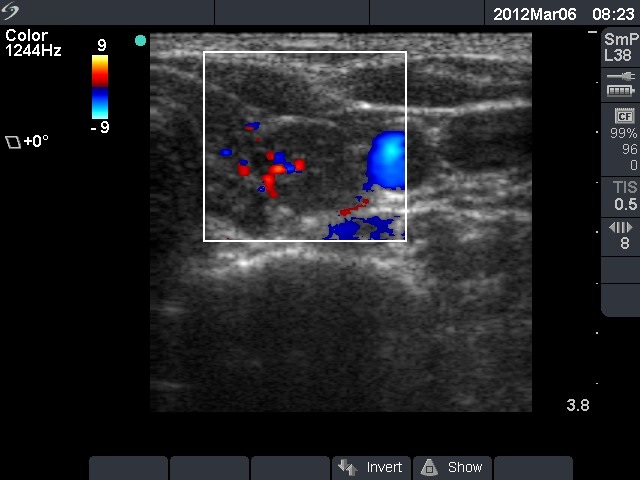
Ultrasonography. The sonographic pattern remained unchanged. The thyroids were hypoechogenic and presented fibrotic changes. There was a more hypoechogenic and less inhomogeneous nodule in the ventral part of the left lobe. The presence of a halo was doubtful as was a type 2 vascular pattern. There were several other, smaller hypoechogenic discrete lesions in both lobes.
Cytological diagnosis: Hashimoto's thyroiditis and suspicion of an oxyphilic tumor with less than 5% estimated risk for carcinoma.
A left lobectomy was performed. Intraoperative frozen section diagnosis indicated a benign lesion.
Histopathology disclosed benign hyperplastic nodules and Hashimoto's thyroiditis.
Comments.
-
Note that the echo structure of the lesion and the extralesional parts of the thyroid are similar. The lesion is presumably a secondary lobule. Nevertheless, the presence of microcalcifications requires a cytological evaluation.
-
It would be very difficult to revise the cytological diagnosis: although there are obvious signs of Hashimoto's thyroiditis, an oxyphilic tumor cannot be excluded.