
|
|
Follicular adenoma - Case 35.
|
|










Clinical data: A 72-year-old woman was referred for evaluation of a nodular goiter. She was treated because of a toxic nodule for 17 years. The patient got thyroid drugs neither prior nor after therapy. She had no complaints after radioiodine therapy, but her thyroid began to increase in the last year and caused already difficulties in swallowing.
Palpation: a hard nodule in the right lobe.
Functional state: euthyroidism with TSH 0.72 mIU/L.
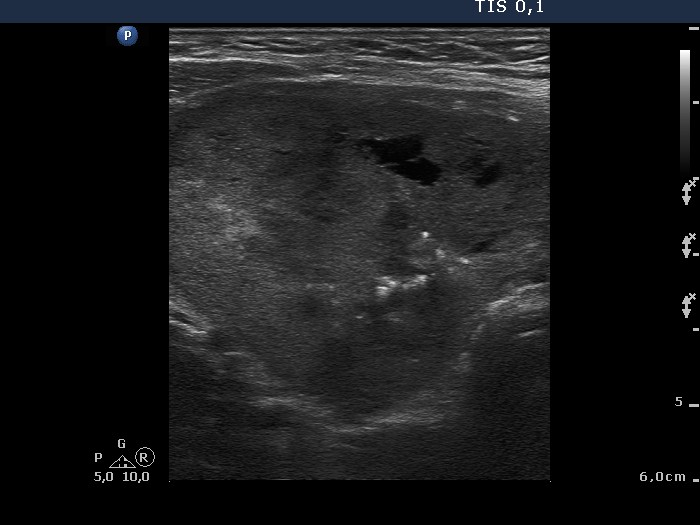
Ultrasonography. A large hypoechogenic nodule occupied almost the entire right lobe. The nodule presented central cystic degeneration and irregular, relatively large hyperechogenic foci. Halo sign was not present while Doppler mode disclosed perinodular blood flow.
Cytology resulted in benign atypia caused by previous radioiodine therapy.
Scintigraphy disclosed less than the average iodine uptake of the nodule. Considering the age of the patient, large dose radioiodine therapy was considered, but it was contraindicated because of the incontinency of the patient. Therefore surgery was performed.
Histopathological diagnosis: dominantly normofollicular adenoma.
Comments:
-
This case demonstrates that Doppler method is superior to gray scale mode in judging sonographic signs of a capsule. The echo structure of the nodule may be identical to that of a capsule in hypoechogenic nodules therefore in such cases we cannot visualize the halo.
-
Hyperthyroidism, radioiodine or thyrostatic therapy may cause significant atypia. If we consider the 8-year cell cycle of the thyrocytes, it is evident that the effect of a radioiodine therapy may last at least a decade. This patient was treated for more than double the average lifetime of a follicular cells. We suppose that ionizing radiation may lengthen this period.
-
If a cytopathologist is faced with thyroid atypia, firstly, he or she has to answer the question: which type of a thyroid carcinoma the atypia may belong to? In this case, the cytological picture excluded anaplastic, medullary and secondary carcinomas of the thyroid. No nuclear properties of a papillary cancer was present. Follicular carcinoma remained the only malignant possibility. Nevertheless, the smear lacked follicular proliferation.