
|
|
Follicular adenoma - Case 32.
|
|












First examination (1st and 2nd rows of images)
Clinical data: a 38-year-old woman with a nodule known for 5 years. Previous FNAC was benign.
Palpation: a moderately firm nodule within the right lobe.
Functional state: euthyroidism with TSH 1.10 mIU/L.
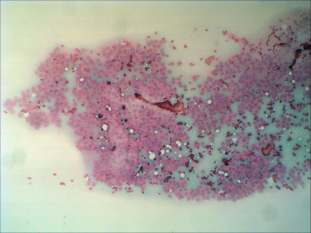
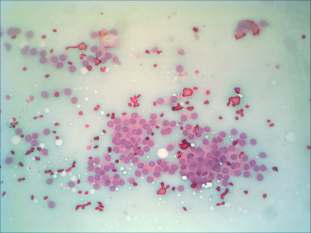
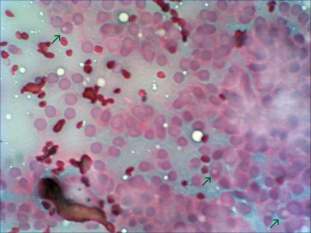
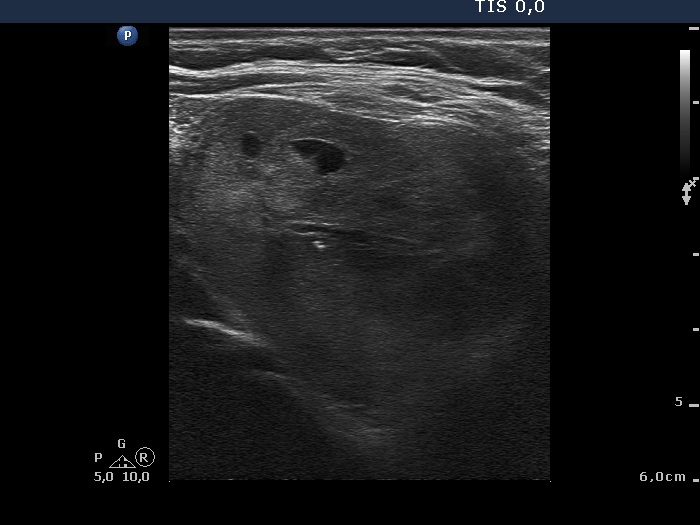
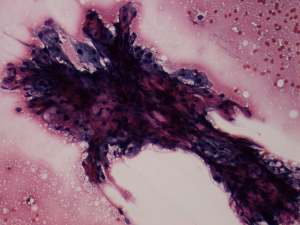
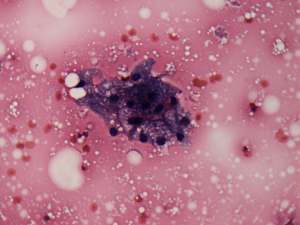
Ultrasonography: a moderately hypoechogenic nodule in the right lobe. Neither halo sign nor perinodular blood flow was present. The dimensions of the nodule were 35x31x37 mm.Cytological picture of the nodule in the right lobe: no colloid in the background. Thyrocytes are arranged in monolayered sheets and in papillary structures composed of microfollicles. Follicular cells are of even size. A few intranuclear holes are present, but these are only projections of vacuoles seen in other parts of the smear, as well. There is no significant atypia.
Cytological diagnosis: tumor with follicular structure.
We offered surgery because of the size of the nodule. But the patient did not accept our suggestion.
Repeat examination 7 years later (3rd and 4th rows of images)
Clinical data: the patient had complaints in supine position for half a year.
Palpation: a moderately firm nodule within the right lobe.
Functional state: euthyroidism with TSH 2.98 mIU/L.
Ultrasonography: the nodule in the right lobe significantly increased in size. The presence of a halo and a type 2 vascular pattern were doubtful. The dimensions of the nodule were 42x38x49 mm which were significantly greater than those on previous investigation. There was a small hypoechogenic lesion in the left lobe.
Cytology was performed from the lesion in the left lobe and resulted in benign, colloid goiter.Cytological diagnosis: benign, colloid goiter.
Right lobectomy was performed. Histopathology: revealed follicular adenoma.
Comments.
-
The correct interpretation of intranuclear holes is very important in this case. Otherwise, the possibility of a follicular variant of papillary cancer could be raised, because no sonographic signs of a capsule could be detected.
-
We use the term benign follicular proliferation in patterns presented by the right lobe. The risk of a follicular carcinoma is around 1% in such cases in our moderately iodine-deficient region.
-
To repeat the FNAC from the right nodule had only very limited sense because it did not influence the further therapy. On the other hand, we aspirated the lesion in the left lobe in order to prove that this lesion is benign and therefore the patient could avoid an unnecessary bilateral surgery.