
|
|
Papillary carcinoma - Case 68.
|
|



Clinical data: a 68-year-old woman followed up for 10 years because of Hashimoto's thyroiditis. On the last occasion, 2 years before present investigation she was euthyroid with a TSH 1.62 mIU/L. The patient noticed a sudden increase of a nodule in the middle of the neck over the last 2 months.
Palpation: a very hard, not freely moveable nodule in the isthmic part of the thyroid.
Functional state: hypothyroidism with TSH 13.4 mIU/L, FT4 7.11 pM/L, aTPO 1022 U/mL, anti-hTG 1215 U/ml.
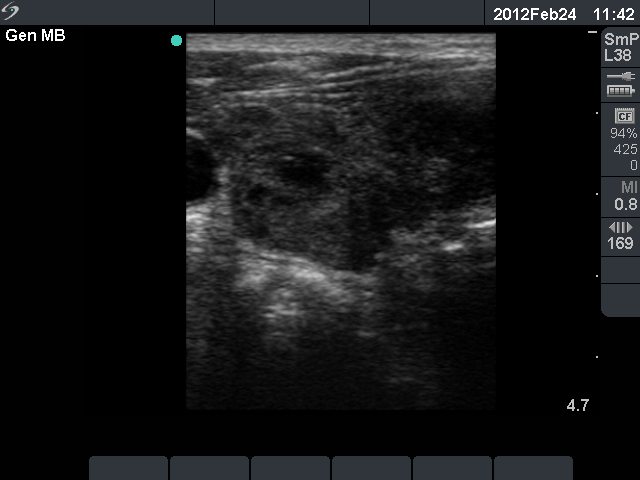
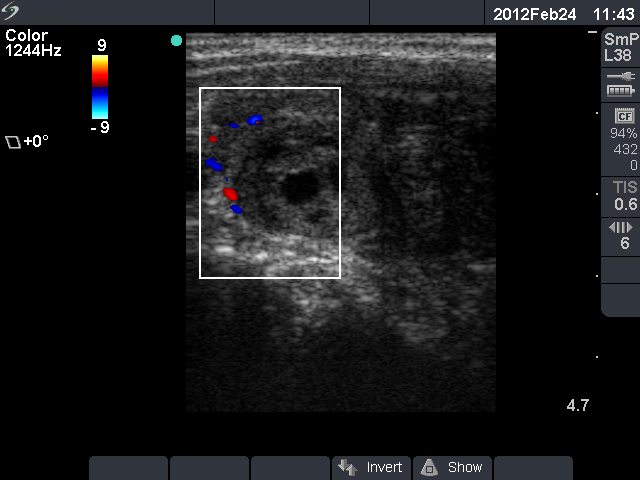
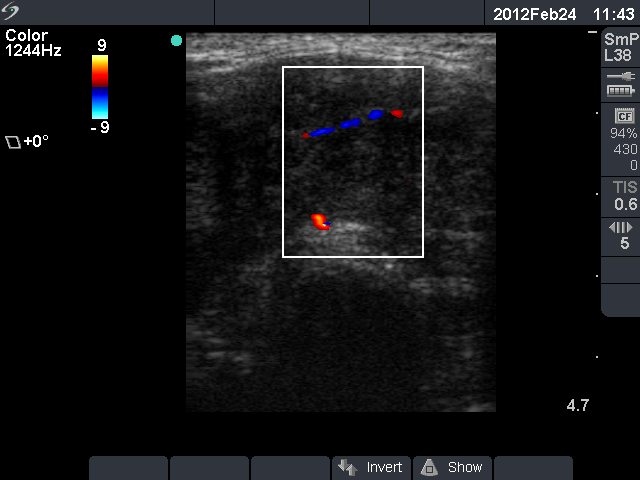
Ultrasonography: the echo structure of the thyroid lobes was identical with previously seen pattern; both lobes were moderately enlarged, hypoechogenic and contained multiple discrete lesions. There was a large hypoechogenic lesion in the isthmus with more pronounced hypoechogenicity than that of the extralesional part.
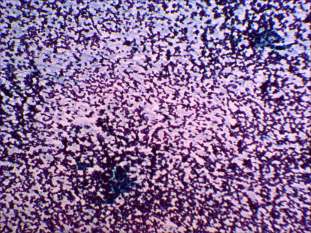
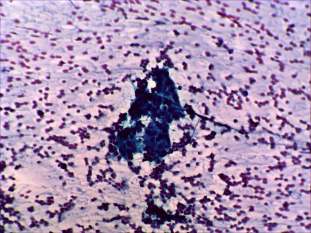
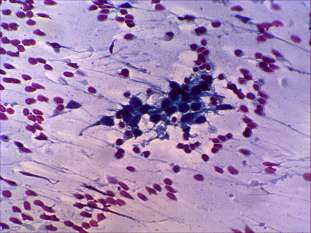
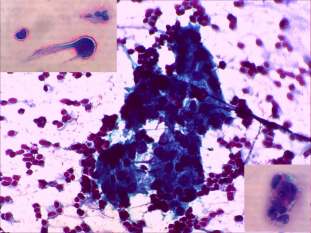
Cytology. There was no colloid in the background. We found small cohesive groups of follicular cells with nuclear crowding and overlapping. Follicular cells exhibited oxyphilic metaplasia. There were a few atypical pleomorphic cells on the smear. Cytological diagnosis: suspicion of anaplastic carcinoma.
The patient was operated on. The frozen section diagnosis was anaplastic carcinoma.
Final histopathology. Benign hyperplastic nodules. Hashimoto's thyroiditis. Two focuses of oxyphilic variant of papillary carcinoma within the isthmic part with 3 and 4 mm in maximal diameter, respectively. No metastatic focuses in the 12 lymph nodes investigated.
Comments. The fundamental statement: we have no other way to trust to the golden standard, to the final result of histopathology.
-
This is one of the very few cases in our practice where the clinical picture was absolutely deceiving. The clinical presentation was identical with that observed in anaplastic cancer. The extreme rapid development (i.e. within one or two months) of a fixed very hard goiter - this is a very specific pattern of anaplastic cancer. Only two exceptions occurred in our more than 20 years practice with more than 120,000 thyroid patients.
-
MALT-type lymphoma of the thyroid was the only disease which had to taken into consideration. Nevertheless, the clinical presentation argued against this possibility because this malignant disease evolves over 3 to 8 months, and although presents as a hard, not freely moveable nodule, this patient had an almost stone-hard lesion. Naturally, the underlying Hashimoto's thyroiditis known for a decade could argue for the possibility of a MALT-type lymphoma.
-
The cytological picture excluded the possibility of a lymphoma. We did not meet any case of MALT-lymphoma which would not be extremely cellular. There were practically no lymphoid cells on the smear. On the other hand the presence of only scattered number of atypical cells is a frequent situation in the case of anaplastic cancer.
-
Considering the final histopathology, we have serious doubt about the origin of the cells seen on the smears which are demonstrated on the cytological images here. The ratio of volume of the carcinoma to that of the whole lesion was in the range of 1:500 to 1:1000.
-
Last but not least. The fundamental, the trust to final histopathology was confirmed on follow-up of the patient. The patient underwent total thyroidectomy, and did not get radioiodine treatment. 14 months after the operation, the patient is well and disease free on daily 125 microgram levo-tiroxine therapy.