
|
|
Benign nodular hyperplasia - Case 56.
|
|










Clinical presentation: a 74-year-old woman was referred for evaluation of a nodular goiter detected on thoracic CT scan. The patient was operated on adenocarcinoma of the lung for 2 years. She had no complaints suggesting a thyroid dysfunction.
Palpation: the right thyroid was enlarged and contained multiple nodules on palpation.
Ultrasonography. The right thyroid was significantly enlarged and contained multiple nodules with different echogenicity. The left thyroid was decreased in size and presented small insignificant lesions.
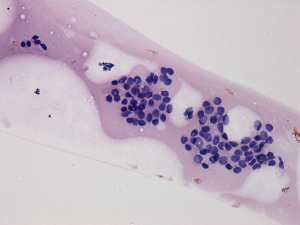
Cytology was performed from one of the mixed nodules in the right lobe and resulted in benign lesion corresponding to hyperthyroid goiter.
Functional state: hyperthyroidism (TSH undetectable, FT4 28.1 pM/l).
Scintigraphy disclosed an autonomously functioning nodule with a maximal diameter of 5 cm in the right lobe.
We administered methimazole therapy and the patient underwent on right lobectomy.
Histopathology disclosed benign hyperplastic nodules with degenerative changes and a solitary focus of papillary microcarcinoma with 6 mm in maximal diameter.
Comment.
-
The essence of our evaluation protocol is the performance of all investigations at first visit. It means that we perform ultrasonography and aspiration cytology and we send the patient for blood test if the latter was not made before our examination. This manner may have disadvantages in those patients who prove to be hyperthyroid because in such patients the aspiration cytology may be superfluous.
-
The cytological pattern is characteristic of hyperthyroidism. The sonographic presentation is characteristic of a toxic multinodular goiter because of the shrinkage of the contralateral lobe caused by the low TSH level.