
|
|
Benign nodular hyperplasia - Case 25.
|
|






Clinical presentation: a 43-year-old woman requested an evaluation of a thyroid nodule discovered one year earlier.
Palpation: the right lobe was enlarged and a large nodule was palpable.
Result of blood test: euthyroidism with TSH-level 0.51 mIU/L.
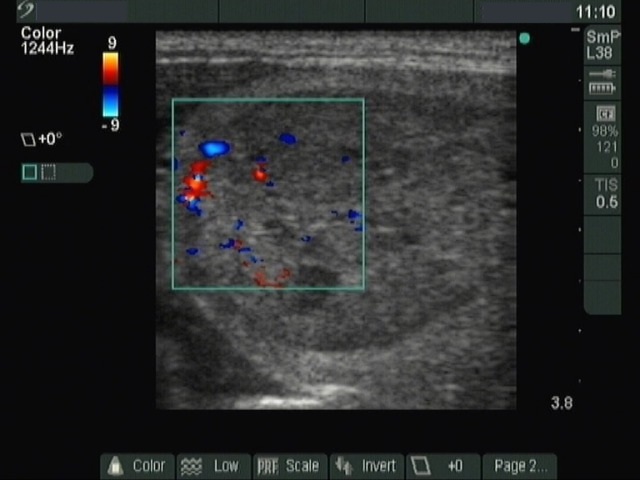
Ultrasonography: a moderately hypoechogenic, inhomogeneous nodule with microcalcifications was present in the right lobe. Halo sign and perinodular blood flow could be detected. The left lobe was echonormal and small.
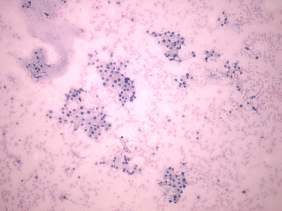
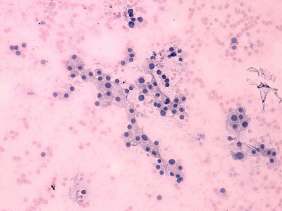
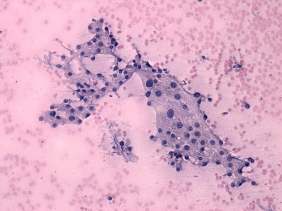
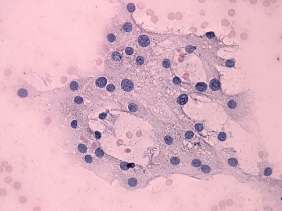
Cytological picture: there is no colloid in the background. Thyrocytes are found in monolayered sheets. There is pronounced anisonucleosis, but no pleomorphism. Follicular cells have small prominent nucleoli.
Preliminary combined cytological-sonographic diagnosis: benign, follicular adenoma with great probability.
Scintigraphy indicated autonomously functioning adenoma.
The patient underwent right lobectomy.
Histopathology: benign hyperplastic nodule. A solitary focus of papillary carcinoma with a maximal diameter of 4 mm.
Comment: the nodule was greater than 4 cm in maximal diameter. In most of such large autonomously functioning adenomas, the TSH is at least decreased (in more than 92% in our practice). Nevertheless, the sonographic appearance of the nodule and the small size of the contralateral lobe are specific signs of toxic nodule. Naturally, if we knew that the nodule is toxic, we would not perform FNAC