
|
|
Benign nodular hyperplasia - Case 26.
|
|









Clinical presentation: a 61-year-old man with vertigo was referred for an examination because of a thyroid nodule found on neck ultrasound examination.
Palpation: a firm nodule in the isthmic part of the left lobe.
Functional state: euthyroidism.
Ultrasonography: a hypoechogenic nodule with dimensions 29x24x33 mm. The nodule presented neither halo sign, nor perinodular blood flow.
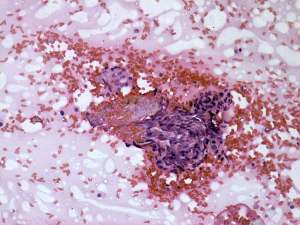
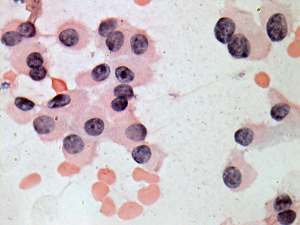
Cytological pattern corresponded to a Hürthle-cell tumor.
Combined cytological-sonographic report benign nodule displaying oxyphilic changes with great probability. The risk of malignancy is less than 1%.
We suggested follow-up and surgery if the nodule would later increase in size.
The daughter of the patient searched for "Hürthle-cell" on the net and requested a second opinion in another institute where a diagnosis of suspicion of oxyphilic cell carcinoma was given.
Histopathology: disclosed benign, hyperplastic nodular goiter.
Comments.
-
The cytological pattern is an example of our limitation of cytological ability. This pattern is identical to that seen in an oxyphilic tumor. The lack of nuclear inclusions and grooves practically excludes the possibility of an oxyphilic variant of papillary carcinoma.
-
Although the lack of sonographic signs of a capsule stood against the possibility of a follicular-type tumor, we has to consider the fact that 5% of follicular tumors lack these sonographic properties. Taking all of these into account I think that in such cases the follow-up of the patient is a safe method.
-
Naturally, if we follow the current protocol this patient has to be operated on. This case illustrates why to change our behavior, the role of sonography has to be changed. Now the only role of ultrasound is in the selection of patients for cytology. If we took the sonographic results into account we can reach better results compared with the current method when we decide solely on cytological findings.