
|
|
Benign nodular hyperplasia - Case 36.
|
|




Clinical presentation: a 61-year-old woman was referred for a second opinion. She was operated on multinodular goiter 18 years earlier. A recurrent nodule was discovered on a routine examination. The FNAC report was "suspicion of follicular variant of papillary cancer".
Palpation: no abnormalities.
Functional state: euthyroidism.
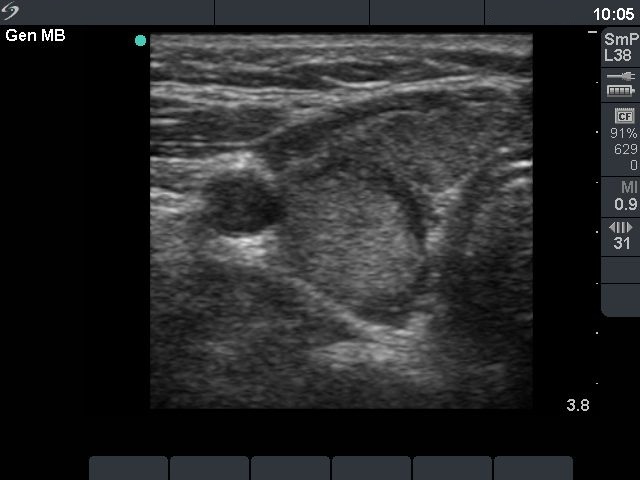
Ultrasonography: there was a hyperechogenic nodule with a halo sign in the right thyroid.
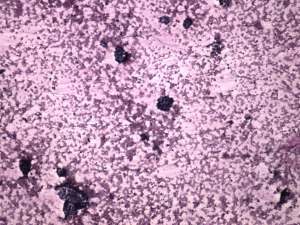
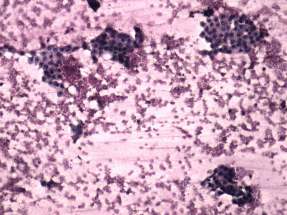
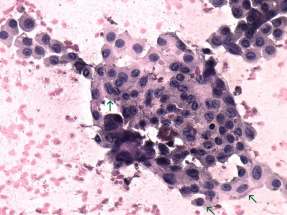
Cytological report: benign follicular proliferation.
The combined clinical-sonographic-cytological report: benign recurrent nodule with the risk of malignancy less than 1:100.
I advised her not to undergo an operation but continue the yearly follow-up examinations. The patient looked for a third physician, who offered surgery.
Histopathology: revealed benign hyperplastic nodule.
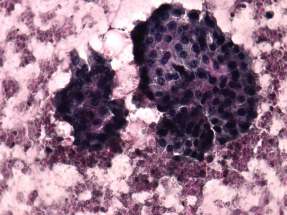
Comment. Recurrent nodules in previously operated patients are almost exclusively benign. The patient had a hyperechogenic nodule. Furthermore, the cytological picture is consistent with that seen in follicular tumor or hyperplastic nodule with follicular proliferation. Nuclear details resembling papillary cancer were present, but these were probably artifacts (see comment to the 4th cytological picture). Moreover, we must be aware about the advantages and disadvantages of surgery. If this patient was regularly controlled, and if her nodule did not increase later, she could avoid the increased complication rate of an unnecessary surgery. Conversely, if she had a cancer, this malignancy would be a well-differentiated one. In this case the patient would be operated one or two years later because of her nodule growth. To the best of our knowledge, even a few year delay in the appropriate therapy has no harm in such cases.