
|
|
Benign nodular hyperplasia - Case 54.
|
|










Clinical presentation: a 59-year-old man was investigated because of neck discomfort lasting for a half year. A large nodule was found in the left lobe. Scintigraphy disclosed a "cold" nodule. He was referred for aspiration cytology.
Palpation: a large firm nodule in the left lobe.
Functional state: euthyroidism (TSH 0.34 mIU/L).
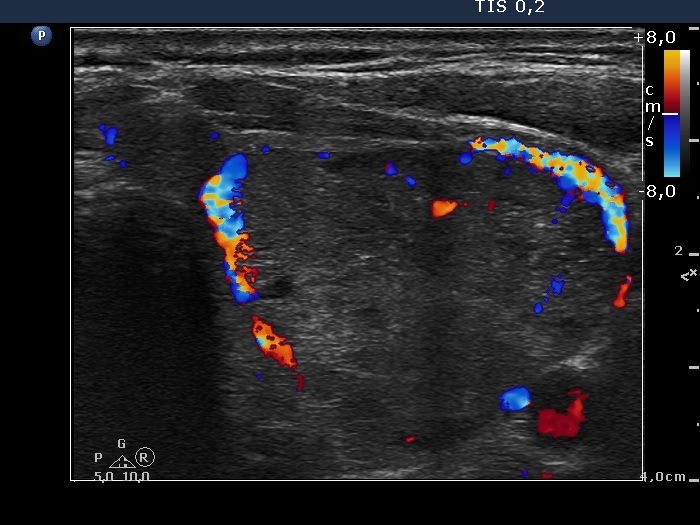
Ultrasonography. The right thyroid was intact. A large nodular area occupied almost the entire left thyroid. It was composed of moderately hypoechogenic, cystic, echonormal and hyperechogenic discrete lesions. The whole lesion was surrounded with an incomplete halo and presented a type 2 vascular pattern.
On the cytological pattern an oxyphilic tumor or an oxyphilic variant of papillary carcinoma could not be excluded.
We gave a final, combined sonographic-cytological diagnosis: benign cystic-colloid goiter with oxyphilic metaplasia. The risk of carcinoma except for a microcarcinoma is less than 1%.
Histopathology disclosed benign hyperplastic nodules with degenerative changes.
Comments.
-
This case points to the inconsistency of Bethesda system. We gained 5 smears from the nodule. In one of them presented in the case study we found atypical cells. There were no follicular cells on two other smears while macrophages and a few thyrocytes were found on the fourth and a pattern of colloid goiter on the fifth smear. If we followed the suggestion of Bethesda system we performed another FNAC months later. What would be the chance that we will target a possible malignant small focus on this second occasion? And conversely, could we feel reassured if we do not find atypical cells on the next occasion?
-
The sonographic pattern, i.e. a large nodular area composed of discrete lesions with different echogenicity is characteristic of a benign, hyperplastic nodule.
-
The cytological pattern itself is suspicious for a carcinoma, either of a Hürthle-cell tumor or a Hürthle-cell variant of papillary carcinoma. Nevertheless, we took the sonographic pattern into account and gave a final combined cytological-sonographic diagnosis described above. The sonographic pattern practically excluded that the whole nodular lesion would be a papillary carcinoma. A Hürthle-cell variant of a follicular carcinoma should be considered. However, the sonographic pattern stands against this possibility. The halo sign was incomplete and the pattern of numerous discrete lesions within the nodular area did not fit a follicular carcinoma. Taking all these into account, we could not exclude the possibility that there was a small focus of an oxyphilic variant of papillary carcinoma within the nodule, but the chance that the whole lesion would be a carcinoma could be excluded.