
|
|
Papillary carcinoma - Case 39.
|
|

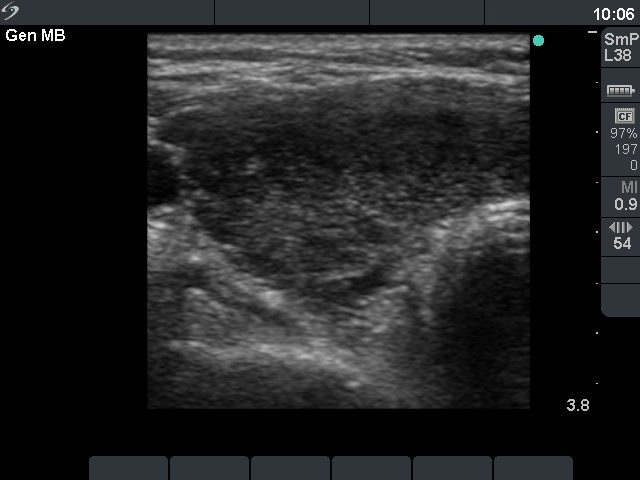
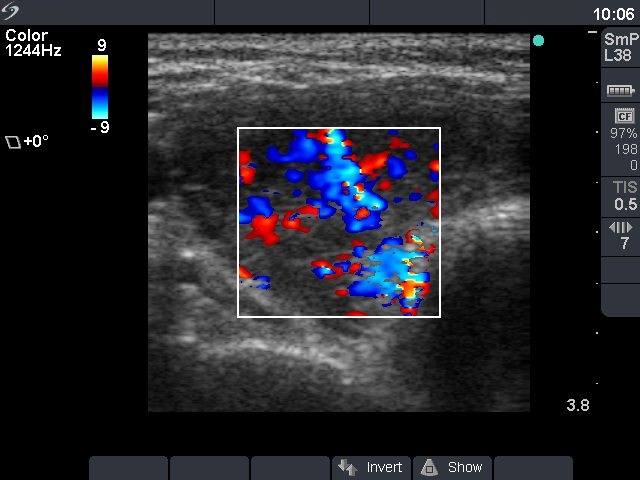







First examination (first row of ultrasound images)
Clinical data: a 37-year-old woman was referred for an evaluation of typical complaints suggesting hyperthyroidism and signs of mild thyroid associated orbitopathy.
Palpation: both thyroids were enlarged.
Functional state: hyperthyroidism (TSH undetectable, FT4 above 75 pM/L).
Ultrasonography: the thyroid was diffusely hypoechogenic without any nodule. The vascularization was increased.Thyrostatic drug was administered and the patient went on regular follow-up examinations.
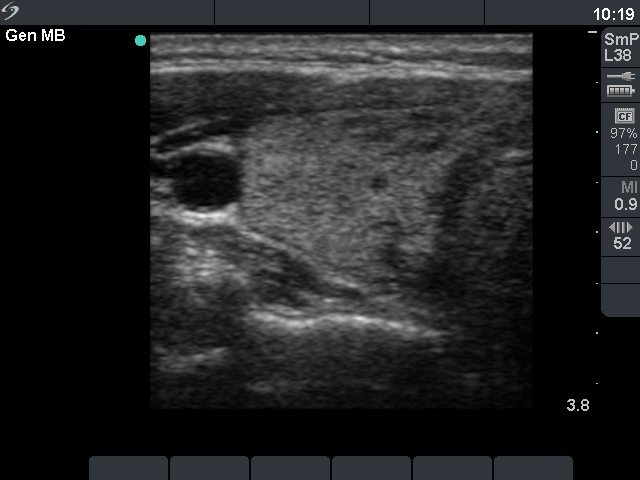
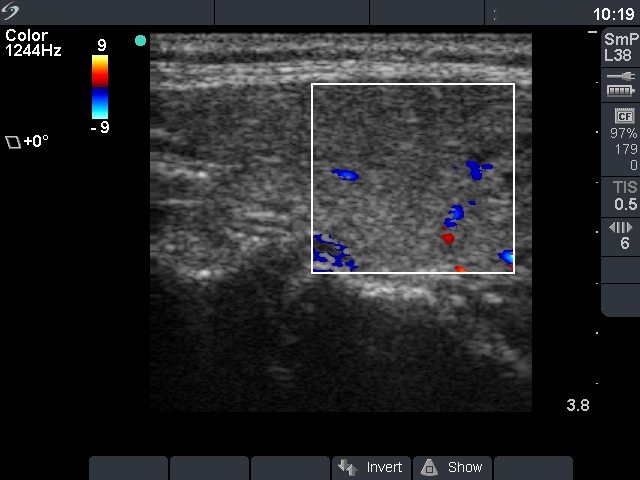
Follow-up examination 13 months later (second row of sonographic images and the cytological pictures)
Clinical presentation : the patient was well. We wanted to discontinue the medical therapy.
Palpation : no abnormality.
Functional state: euthyroidism on daily 5 mg methimazole and 50 microgram levo-tiroxin (TSH 2.99 mIU/L, FT4 13.7 pM/L).
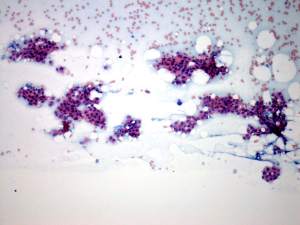
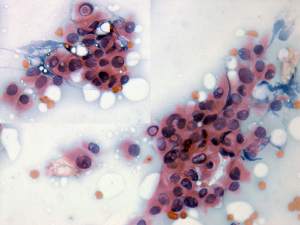
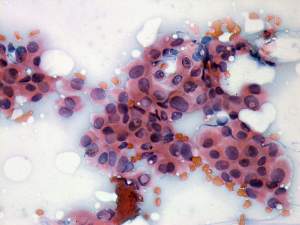
Ultrasonography: compared with the former examination both the size, the echogenicity and the vascularization had normalized except for small hypoechogenic areas with less than 10% of echogenicity index. However, a hypoechogenic nodule with microcalcifications and irregular borders appeared in the left lobe.Cytological picture: there isn't any colloid on the smear. Thyrocytes in irregular clusters with nuclear crowding and overlapping. Thyrocytes are enlarged. Many follicular cells exhibit groove and inclusion. Cytological diagnosis: papillary cancer.
Histopathology: papillary cancer.
Comment: in our practice this was the third patient with a coexistent Graves' disease and papillary cancer in whom we could not detect the focus of papillary cancer on the first examination. The basic echo structure in the active phase of the autoimmune process was identical with the focus of papillary cancer, therefore the nodule was hidden. The only chance to detect the carcinoma is to repeat ultrasonography until the basic echo structure will be normalized.