
|
|
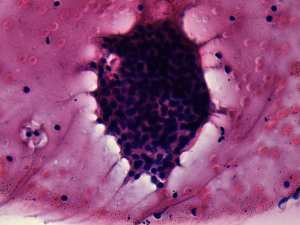
Benign nodular hyperplasia - Case 20.
|
|




Clinical presentation: a 36-year-old woman was referred for an evaluation of elevated TSH-level detected on a routine examination.
Palpation: no abnormality.
Functional state: subclinical hypothyroidism (TSH 5.13 mIU/L, FT4 14.1 pM/L).
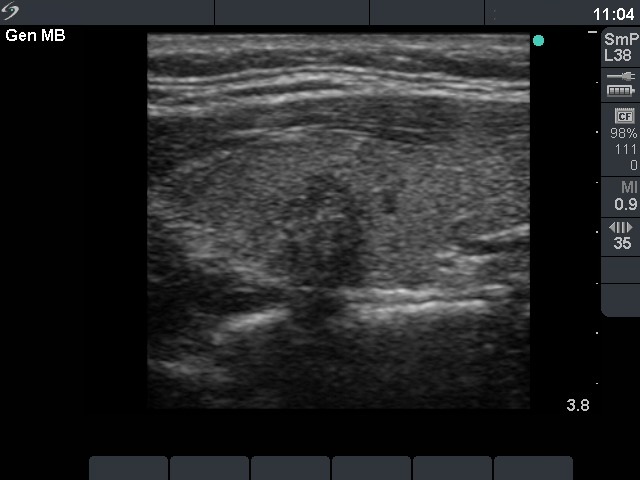
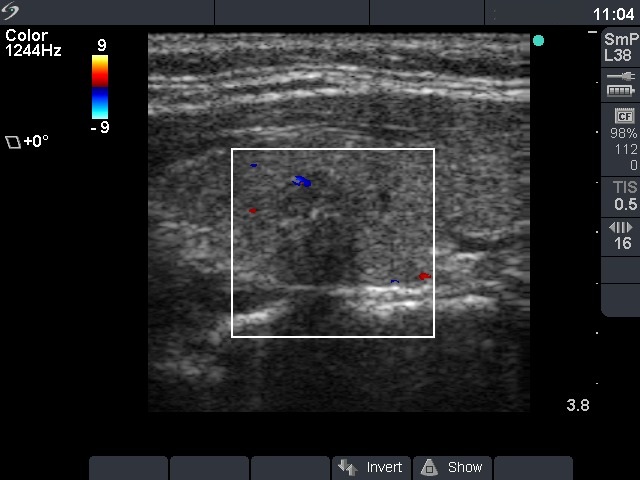
Ultrasonography: the thyroids were echonormal. There was a small moderately hypoechogenic lesion in the left lobe. The nodule displayed microcalcifications and had blurred borders.
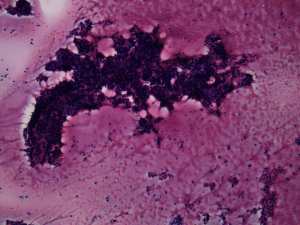
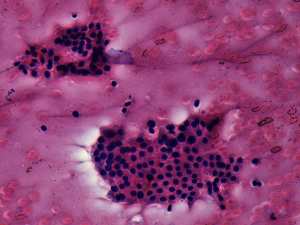
Cytological diagnosis: benign colloid goiter.
Anti-TPO was performed and resulted in normal value (2 U/mL).
We suggested follow-up. 3 months later and thereafter in the next 2 years during pregnancy and lactation the TSH was in the range of 0.8-2.7 mIU/L. 2 years after the initial examination the volume of the nodule was 85% of the original.
Comments:
-
If previous ablative therapy and de Quervain's thyroiditis are excluded, the cause for hypothyroidism is autoimmune thyroiditis in most if not all cases in an adult person. Lymphocytic thyroiditis has a very specific ultrasound pattern, i.e. various degree of hypoechogenicity. In the event of an echonormal thyroid and elevated TSH-level, the failure of the laboratory test has to be considered.
-
The ultrasound pattern was suspicious for a papillary cancer. The combination of hypoechogenicity, irregular borders, the presence of microcalcifications and the taller-than-wide sign increased the risk of malignancy to more than 10-fold. In our minimally-moderately iodine deficient region, it means that instead of a 2.2% risk the patient had a 25% risk for malignancy.