Hashimoto's thyroiditis (cytological diagnosis) - case 1137 |
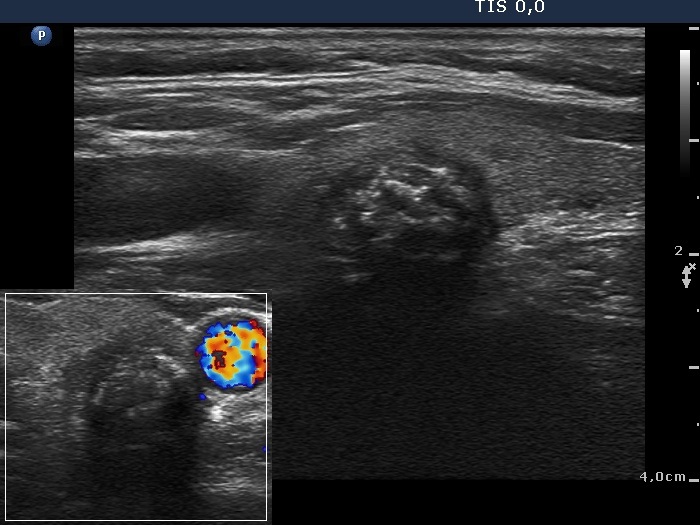
Papillary carcinoma (histological diagnosis) - case 1627 |
 |
 |
|
 |
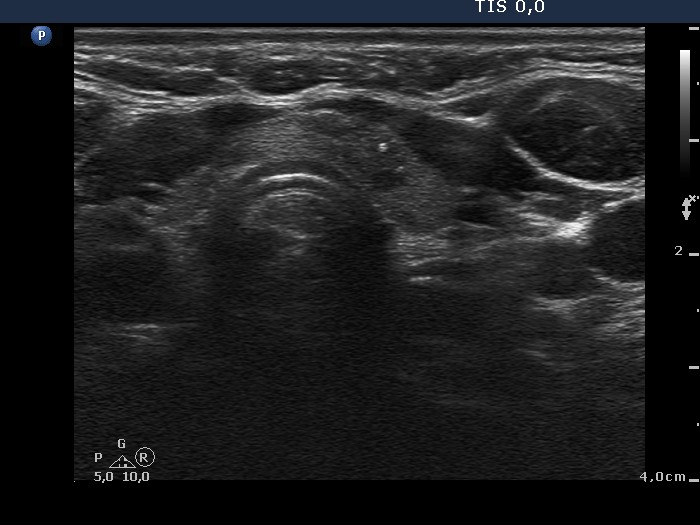
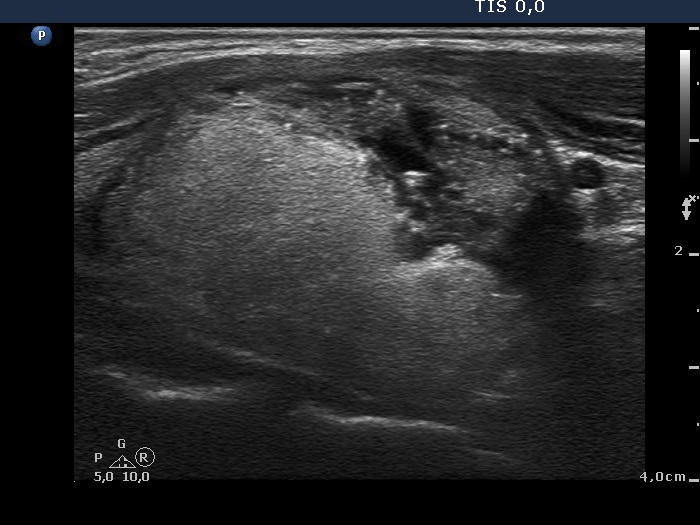
The lesion lacks hyperechogenic figures. The borders are sharp and puzzle-like, a frequent finding in hypoechogenic discrete areas of Hashimoto's thyroiditis.
|
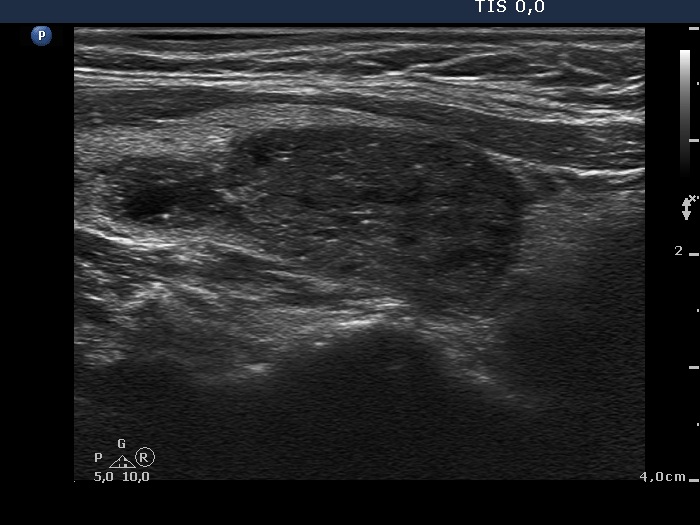
There are two pale figures in the dorsal part of the lesion. It was very hard to decide even analyzing the video whether this figure is a line or two or three tiny granules next to each other. However, the nodule has two additional suspicious features: the taller-than-wide sign and the blurred borders.
|
| |
|
Oxyphilic adenoma - case 60 |
Papillary carcinoma |
 |
 |
 |
 |
There are similar figures in both cases: beside the connective tissue, punctate echogenic foci are found as bright hyperechogenic granules. Although, the ultrasound presentation sharply differs in these two cases: the benign lesion has regular shape and sharp borders while the malignant lesion has irregular shape and blurred borders.
|
| |
|
Intrathyroidal parathyroid adenoma (histological diagnosis) - case 1399 |
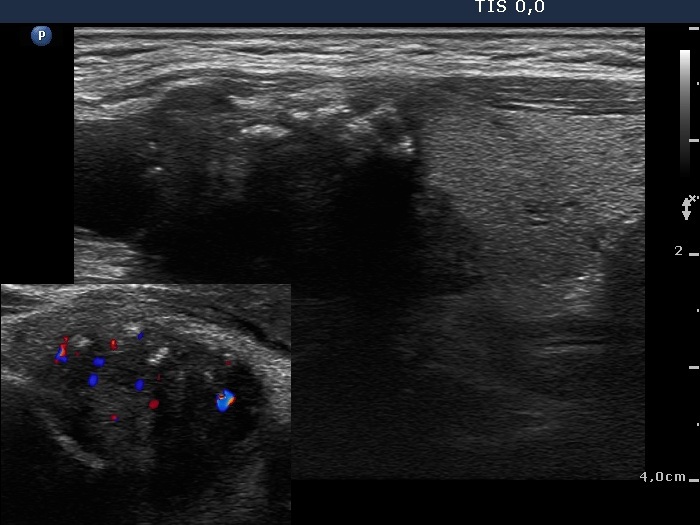
Papillary carcinoma (histological diagnosis) - case conp 031 |
 |
 |
|
 |
There are a few hyperechogenic granules within the small parathyroid lesion and we can see two much thinner lines, as well. These figures might be either punctate echogenic foci or non-specific granules. The papillary carcinoma contains punctate echogenic foci. The main differences between the appearance of the cases are the shape and borders: regular and sharp in the left benign, while irregular, blurred in the right malignant focus.
|
| |
|
|
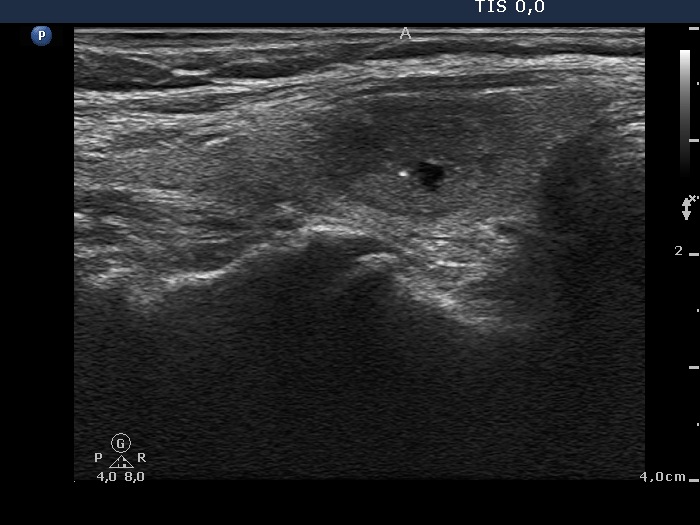
Papillary carcinoma (histological diagnosis) - case conp 035 |
 |
 |
 |
 |
The thyroid presented in the left images is composed of moderately hypoechogenic and hypoechogenic nodules, while the lobe in the malignant case is diffusely hypoechogenic and has a less hypoechogenic but more inhomogeneous lesion in its dorsal part. Both the left thyroid and the malignant nodule in the right images have hyperechogenic granules and lines which correspond to a connective tissue.
|
| |
|
Benign hyperplastic nodules (histological diagnosis) - case 444 |
Papillary carcinoma (histological diagnosis) - case p002 |
 |
 |
 |
 |
Both lesions contain bright granules and lines, i.e. proliferation of connective tissue. The simultaneous presence of punctate echogenic foci (microcalcifications) cannot be excluded in either case. The ultrasound presentation differs in the shape and borders of the nodules. In contrast with the benign lesion, the malignant nodule is lobulated and has blurred borders in its dorsal part.
|
| |
|
Oxyphilic adenoma (histological diagnosis) - case 1735 |
Papillary carcinoma (histological diagnosis) |
 |
 |
 |
 |
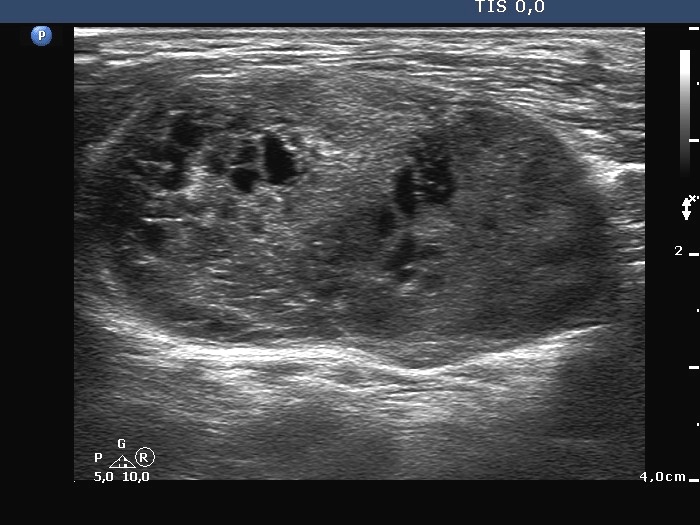
Both lesions have multiple cystic areas. The malignant case clearly belongs to spongiform cyst category because the cystic area exceeds 50% of the nodule. The risk of malignancy is very low in such lesions if there are no signs suggesting an increased risk. The solid part was hypoechogenic in these cases therefore aspiration cytology was mandatory. Note that both cases presented signs of posterior acoustic enhancement, i.e. hyperechogenic figures in the back wall of the microcystic areas. There was only one but an important difference between the cases. The benign nodule was located within the thyroid, while the malignant was found in a lateral aberrant thyroid tissue.
|
| |
|
Benign hyperplastic nodule (histological diagnosis) - case 80 |
Papillary carcinoma (histological diagnosis) - case p057 |
 |
 |
 |
 |
The two cases differ in the lack and presence of punctate echogenic foci, benign (left) and malignant (right) case, respectively.
|
| |
|
Benign hyperplastic nodule (histological diagnosis) - case 1091 |
Benign hyperplastic nodule (histological diagnosis) - case p026 |
 |
 |
 |
 |
Both spongiform cysts present hyperechogenic figures including fibrosis and posterior back wall enhancement, the left benign lesion does comet-tail artifacts, too. Both lesions had to be aspirated because the solid part of them was hypoechogenic. (The left case seems to have blurred borders but this is only an optical artifact because of inappropriate freezing. See video.)
|
| |
|
Bening hyperplastic nodule (histological diagnosis) - case cons 024 |
Papillary carcinoma (histological diagnosis) - case 607 |
 |
 |
 |
 |
Both cases have both hyperechogenic granules and lines, i.e. proliferation of connective tissue, while the carcinoma contains much larger and brighter granules which correspond to punctate echogenic foci (in this case: microcalcifications). However, the main difference between the cases is the shape and borders of the nodules: regular, sharp and irregular, blurred, benign and malignant cases, respectively.
|
| |
|
Follicular adenoma (histological diagnosis) - case 11 |
Papillary carcinoma (histological diagnosis) - case p009 |
 |
 |
 |

|
The two nodules do not differ neither in the presentation of hyperechogenic figures (which might correspond either to connective tissue or punctate echogenic foci) nor in their shape. Moreover, both are blurred.
|
| |
|
Granulation around surgical thread (cytological diagnosis) - case 1343 |
Papillary carcinoma (histological diagnosis) |
 |
 |
 |
 |
There is a minimal if any significant difference between the ultrasound presentations of these cases: both were irregularly shaped and hypoechogenic, both contained various hyperechogenic figures including compound ones composed of echonormal ragged tissue having bright granules. This striking similarity is the cause for the differential diagnostic issue in the event of granulation around surgical thread. Naturally, the patient history decides this issue.
|
| |
|
Granulation around surgical thread (histological diagnosis) - case 411 |
Papillary carcinoma (histological diagnosis) - case 779 |
 |
 |
 |
 |
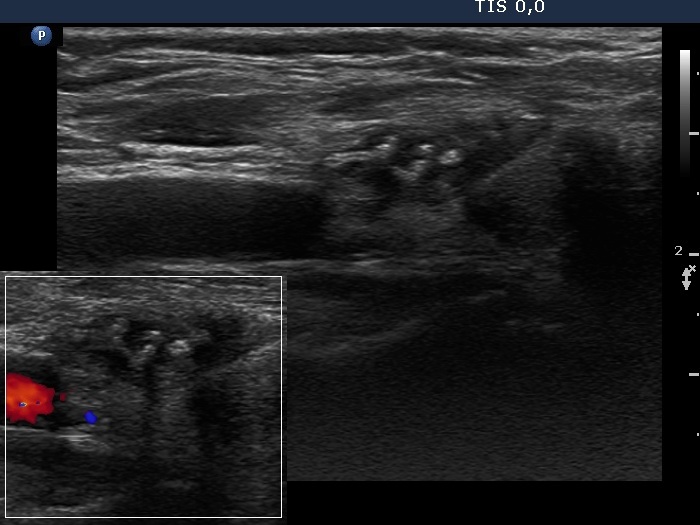
Here is another example of the differential diagnostic problem caused by granulation around surgical thread. Again, there is no difference between the ultrasound presentations of these cases except for the vascularization. The right, malignant case cannot be a granulation around surgical thread which is always avascular; however, this is not a great revelation in a patient who has not been operated. Conversely, the lack of vascularization by no means excludes the possibility of a carcinoma.
|
| |
|
Oxyphilic adenoma (histological diagnosis) - case 368 |
Papillary carcinoma (histological diagnosis) |
 |
 |
 |
 |
The left benign lesion contains a punctate echogenic focus while the right, malignant does proliferation of a connective tissue. The benign lesion has a regular shape and sharp borders, while the malignant nodule has irregular shape and blurred borders.
|
| |
|
|
|
Follicular adenoma (histological diagnosis)
|
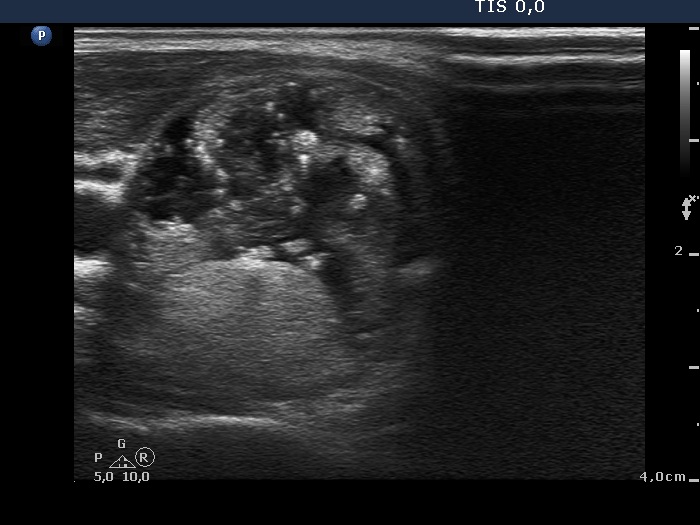
Follicular adenoma (histological diagnosis) - case 424 |
 |
 |
 |
 |
The nodule contains numerous hyperechogenic granules and a few lines and it is possible that the former correspond to punctate echogenic foci, however, the nodule has a regular shape. Nevertheless, the risk of carcinoma is greater compared with an average echonormal nodule.
|
The large spots in the range of 2 to 4 mm are ragged thyroid parenchyma as are most of the smaller similar figures in the upper image. It is reasonable to assume that the smaller granular figures are also ragged parenchyma. On the other hand one of them fulfills the criteria of a comet-tail artifact. The bright granules in the right and upper side of the moderately hypoechogenic part of the lesion are punctate echogenic foci (lower image).
|
| |
|
Follicular adenoma (histological diagnosis) |
Papillary carcinoma (histological diagnosis) - case p027 |
|
 |
|
 |
The nodule presented in the left images has numerous hyperechogenic granules and a few short lines, too. Although we have to consider the possibility that these granules are punctate echogenic foci, the nodule is echonormal and presents halo sign, therefore the risk of a cacinoma is out of the picture and way less compared with the nodule presented in the right images. The latter is hypoechogenic, has a lobulated surface. The hyperechogenic figures within this lesion correspond to proliferation of connective tissue because both hyperechogenic granules and lines occur.
|
| |
| |
| |
| |
| |
|
