
|
|
Benign nodular hyperplasia - Case 12.
|
|






Clinical presentation: a 33-year-old woman was referred for aspiration cytology. A thyroid nodule was detected on an evaluation because of her infertility. FNAC resulted in atypia of unknown significance in another hospital 4 months earlier.
Palpation: a firm nodule in the right lobe.
Functional state: euthyroidism with TSH-level 2.09 mIU/L.
Ultrasonography: there was a minimally-moderately hypoechogenic nodule in the right lobe. The lesion contained tiny, hyperechogenic granules. A type 3 vascular pattern.
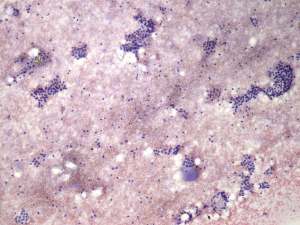
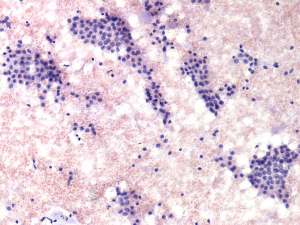
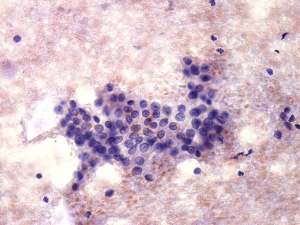
Cytological diagnosis: suspicion of papillary cancer.
Histopathology: benign, hyperplastic nodular goiter.
Comments.
-
It is worth analyzing the hyperechogenic foci within the lesion. The tiny granules are more probably presentations of fibrosis than that of microcalcifications.
-
The cytologic pattern is an example of the limitations of our (my?) knowledge. A great proportion of cells contained grooves.
-
This case reveals one of the basic problems of the new AUS category of Bethesda system. Why do we think that the cytological picture will change over time? And if this pattern becomes reassuring on repeated cytology, how can we exclude the possibility that we aspirated different parts of a nodule, at first a malignant and then secondly a benign part?