|
Follicular adenoma (histology) - case 290 |
Benign hyperplastic nodule (histology) - case 1582 |
 |
 |
 |
 |
 |
 |
|
There is only one important difference between the papillary carcinoma and the two benign cases. The solid part of the former shows an acute angle between the solid part and the cyst' wall while the benign cases present blunt angle.
|
| |
|
|
Benign hyperplastic nodules - case 11 |
 |
 |
 |
 |
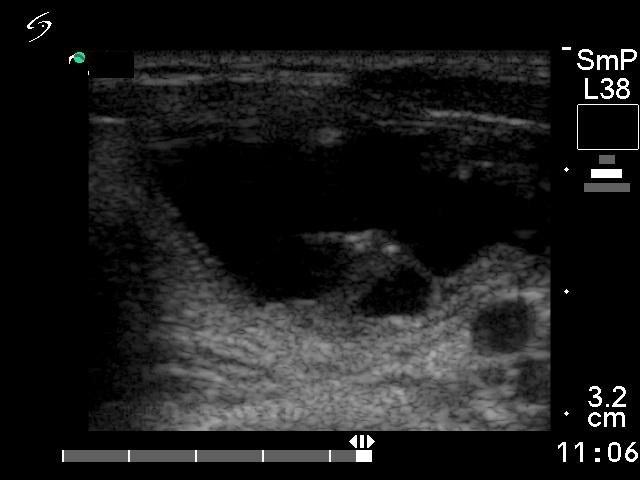
The solid part of both lesions presents projection with lobulated surface. The lobulation has a more limited importance in the event of the solid part of cystic nodules compared with the lobulation of the outer surface of a lesion. As a rule, pathological lobulation always refers to the outer border of a nodule. It is more important that these nodules belong to different subtypes of cystic nodules, the malignant is a peripheral-type while the benign is a central-type cystic lesion. Note the solid rim along the cyst wall in the benign case. The origin of hyperechogenic intralesional figures is doubtful, they may be either non-specific granulations or microcalcifications. The angle between the solid part and the cyst of the wall is even opposite than expected, the carcinoma displays blunt while the benign lesions do acute angle.
|
| |
|
|
|
 |
 |
 |
 |
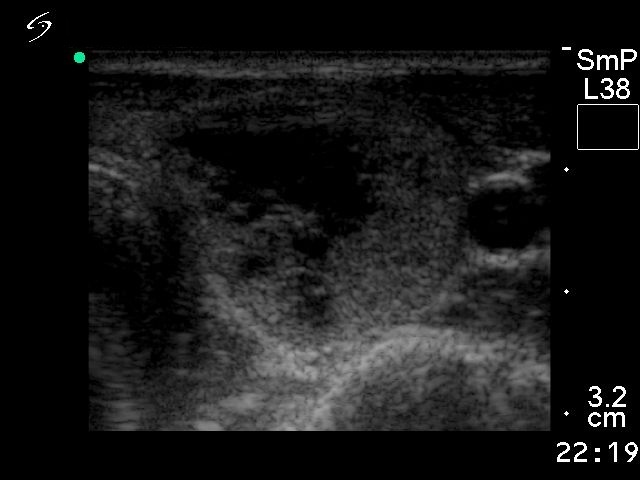
Both nodules are solid lesions which present cystic degeneration. There were two suspicious signs in the event of papillary carcinoma. First, the presence of microcalcification and second, the lobulated margins of the nodule. The presence of fluid deeply alters the basic echogenicity of a nodule, it increases the echogenicity of the solid part. At first sight, the papillary carcinoma seems to be hypoechogenic, but it is caused only by the presence of fluid. Compare the echogenicity of the solid part of the nodule with that of the non-nodular thyroid - these are identically echonormal.
|
| |
|
|
Benign hyperplastic nodules - case 13 |
 |
 |
 |
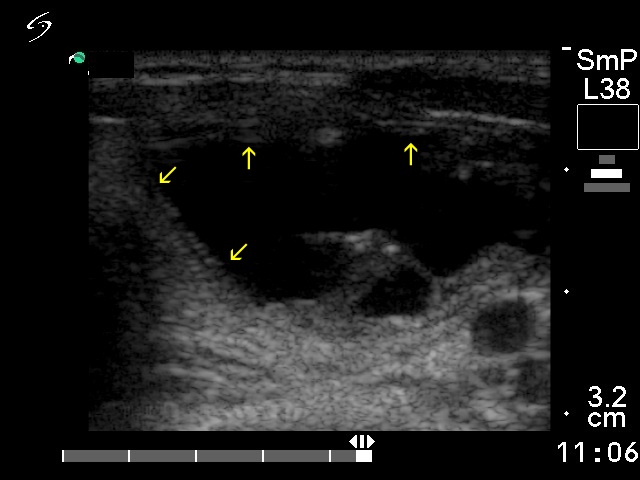 |
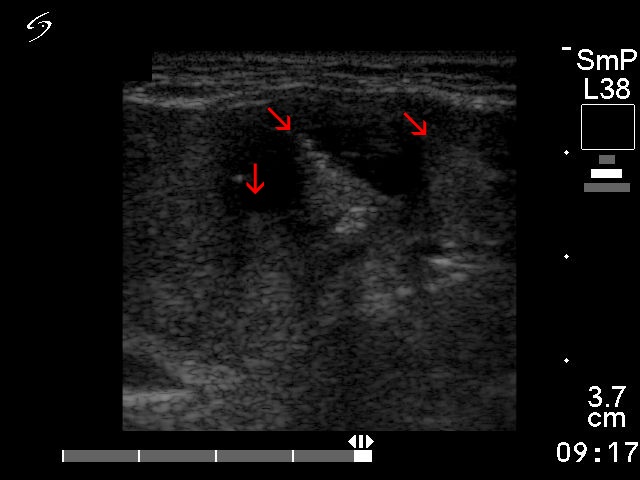
At first sight, both nodules seem to belong to projecting eccentric type. However, solid portions can be observed along the inner wall of the benign lesion (yellow arrows). Therefore, this belongs to the central subtype. The malignant nodule has more projections marked with red arrows.
|
| |
|
|
Benign hyperplastic nodules - case 16 |
 |
|
 |
 |
An eccentric type non-projecting peripheral-type lesion is presented in the left while a central-type cystic nodule in the right case. It is worth comparing the relation of echogenic granules to the cystic areas. The two punctate echogenic foci within the solid part of the malignant nodule are not related to ventral cystic areas, therefore they are probably microcalcifications. On the other hand, all echogenic figures in the right, benign case are located directly behind cystic areas.
|
| |
|
|
|
 |
 |
 |
 |
The malignant nodule is a peripheral-type cystic lesion, while the benign case is a central-type cystic nodule. The solid part of the latter also projects into the cystic cavity. The malignant nodule presents acute while the benign does blunt angles. The cystic degeneration of the solid part is a feature which suggests that the lesion is benign. The interpretation of the echogenic foci in the carcinoma case is difficult, while the echogenic foci in the benign case are clearly related to ventral cystic areas.
|
| |
|
|
Right lobe |
Left lobe |
 |
 |
 |
 |
 |
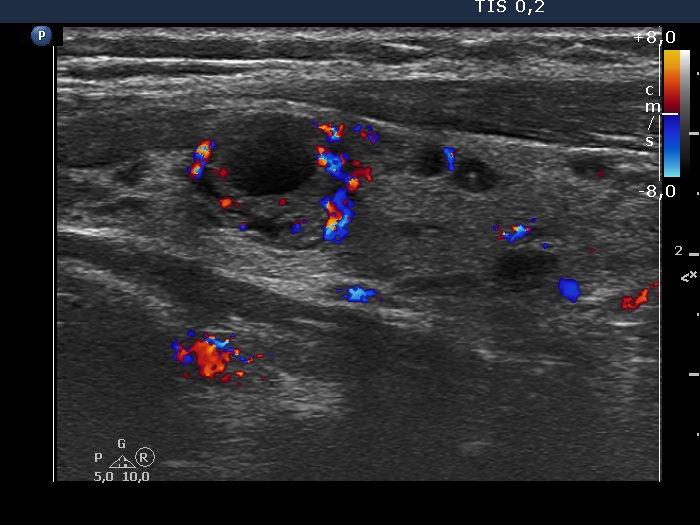 |
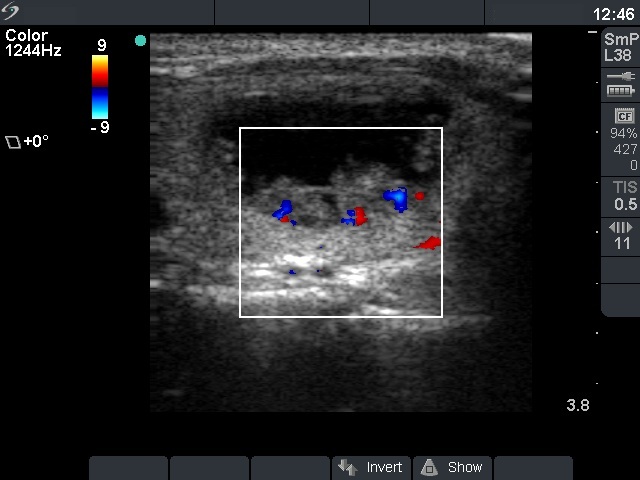
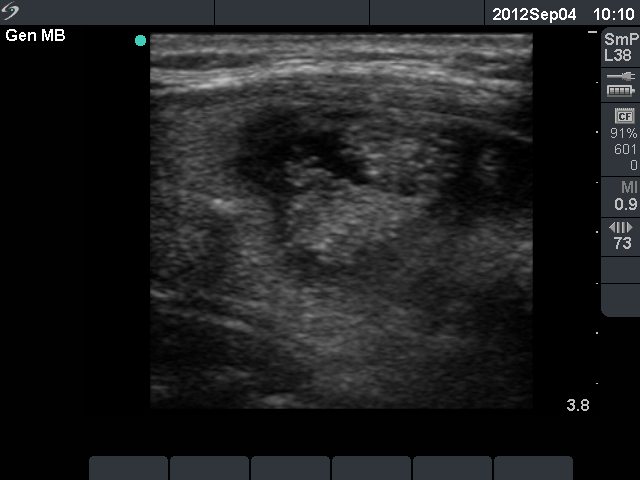
Most lesions presented in this case are dilated macrofollicles and not pathological nodules. The exceptions are those lesions which have solid portions, two in the right lobe and one in the left lobe. The solid parts of these nodules display vascularization.
|
| |
|
|
|
 |
 |
 |
 |
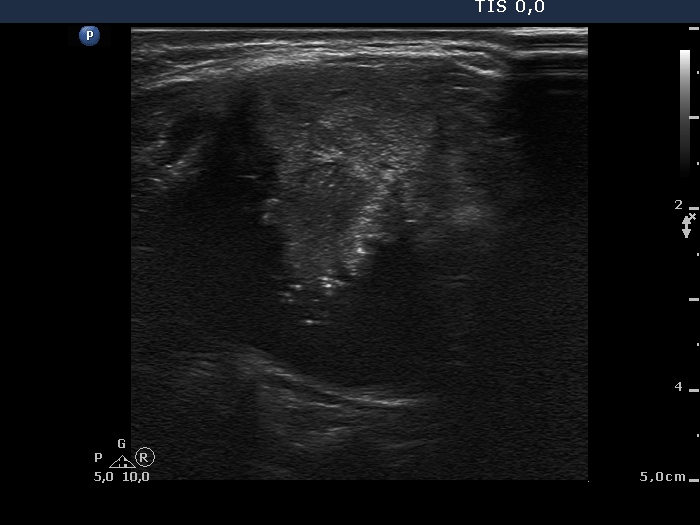
After the aspiration, the composition of the previously seemingly pure cyst has significantly changed: a suspicious solid part has appeared which showed microcalcifications.
|
The dorsal solid part remainde unchanged after evacuation of the cyst. Nevertheless, this is also suspicious because of the presence of hyperechogenic granules.
|
| |
|
|
|
|
|
|
|
The shape of the solid part has no relevance. Compare the appearance of hyperechogenic granules in these cases. The hyperechogenic granules are brighter in the case of papillary carcinoma compared to benign nodules. Nevertheless, this difference does not have enough practical value.
|
| |
|
|
|
 |
|
 |
 |
The only suspicious sign in the malignant case was the moderately hypoechoic pattern of the solid part. Neither the macrolobulation of the solid part nor the presence of echogenic figures are characteristic enough. The border of the solid part has very limited relevance in solid part of a cystic lesion while the echogenic figures are at least in part related to ventral cystic areas. Both cases belong to the peripheral-type of cysts. The vascularization is just the opposite of what we expect: the malignant nodule presents a perinodular while the benign lesion does an intranodular vascular pattern.
|
| |
|
|
Follicular adenoma (histology) - case 486 |
 |
 |
The malignant nodule was a peripheral-type cyst while the benign lesion was a multichambered, central-type cystic lesion. The punctate echogenic foci at the tip of the solid part of the malignant nodule might be microcalcifications while the echogenic figure belong to the back wall cystic subgroup in the adenoma.
|
| |
|
|
|
